You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
INTRODUCTION
Taking patients’ blood pressure during dental examinations is critical to their overall health. High blood pressure is a proven risk factor for cardiovascular disease, heart failure, stroke, and renal (kidney) disease. Many patients see a dentist more frequently than a physician, giving the dental team the responsibility to inform their patients of their blood pressure reading and how it may affect their overall health. Blood pressure should be taken at each recare dental examination, before any procedure on patients with a history of high blood pressure, and before procedures that cause apprehension, such as oral surgery. The patient should always be told what their blood pressure reading is so that they can keep track of differences themselves. Establishing a baseline reading for your patient in a non-stress producing environment produces a more accurate reading if you need to make a medical referral. Screening for blood pressure by the dental professional has proven to be extremely effective since many patients with hypertension may be unaware of their condition.
BLOOD PRESSURE
One in three Americans has high blood pressure or hypertension. Having high blood pressure places your patients at risk for heart disease and stroke. Heart disease is the leading cause of death and stroke is the third-leading cause of death in the United States.
Twenty-five percent of American adults have prehypertension that is higher than normal. Prehypertension raises your patients’ risk for high blood pressure.
Blood pressure is the force exerted by the blood on the blood vessel walls. This force makes a noise called Korotkoff sounds. When the left ventricle of the heart contracts, blood is forced out into the aorta and travels through the large arteries to the smaller arteries, arterioles, and capillaries. During the course of the cardiac cycle, blood pressure is changing constantly.
Systolic pressure is the peak or highest pressure. It is caused when the heart muscle contracts. The normal systolic pressure is less than 120 mm Hg. In patients over 50 years of age, a systolic reading higher than 140 mm Hg is more important as a cardiovascular risk factor than a high diastolic reading.
Diastolic pressure is the lowest pressure. It measures the pressure in the arteries between heartbeats (when the heart muscle is resting between beats and refilling the blood. The normal diastolic pressure is less than 80 mmHg.
Pulse pressure is the difference between the systolic and the diastolic pressures. The normal or safe difference is less than 45 mmHg.
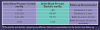
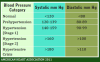
BLOOD PRESSURE CATEGORIES
The American Heart Association recommends blood pressure screening occur starting at age 20. Blood pressure readings defined by the American Heart Association include normal, prehypertension, two stages of hypertension, and hypertensive crisis (See Table 1). Prehypertension is a designation meant to alert patients of a need to intervene and prevent hypertension. Patients in this designation have increasing health risks and need to make major lifestyle changes to return to a normal reading. If changes are not made, prehypertension will progress into hypertension - a serious health risk. Treatment options for hypertension usually require prescription medications and should be discussed, prescribed, and monitored by a physician.
PRIMARY RISK FACTORS THAT INFLUENCE BLOOD PRESSURE
Several risk factors are associated with the development of hypertension. Family history, advanced age, gender-related risk patterns, lack of physical activity, poor diet—especially one that includes too much sodium, overweight and obesity, and drinking too much alcohol are all considered risk factors. In regards to gender-related risks, a higher percentage of men than women have high blood pressure until 45 years of age. After 64 years of age, a much higher percentage of women have high blood pressure than men.
ASSESSMENT FOR IDENTIFIABLE CAUSES OF HYPERTENSION
There are also many conditions or diseases that play a role in hypertension. The medical history should include questions on:
• Sleep apnea
• Drugs being taken that may induce or affect high blood pressure
• Chronic kidney disease
• Renovascular disease
• Cushing’s syndrome or steroid therapy
• Coarctation of aorta (localized narrowing of the aorta)
• Thyroid/parathyroid disease
CONDITIONS WHEN MEASURING BLOOD PRESSURE IN THE DENTAL OFFICE
The National Heart, Lung, and Blood Institute suggest before blood pressure is taken the following conditions should occur at least 30 minutes prior to measurement to provide the most accurate blood pressure reading: no smoking, no exercise, and no coffee or other caffeine.
TYPES OF BLOOD PRESSURE DEVICES
Blood pressure measurement devices are categorized as: manual sphygmomanometers, digital non-portable for upper arm with automatic inflation, digital portable for upper arm with automatic inflation (see Figure 1), digital portable for wrist with automatic inflation, and digital portable for finger with automatic inflation. In a recent Consumer Reports testing (Sept 2008; 47-49) 16 devices were tested with trained medical personnel conducting over 6,000 readings on 57 men and women. The upper arm cuff devices were more accurate than wrist devices. The three highest rated upper arm cuff devices were: Omron Women’s Advanced Elite 7300W, Microlife Deluxe Advanced Automatic #BP3MC1-PC, and Omron Automatic with IntelliSense HEM-711AC.
For manual sphygmomanometers, the sphygmomanometer (blood pressure cuff or machine) consists of an inflatable cuff and two tubes; one tube is connected to the pressure hand control bulb and the other tube to the pressure gauge (see Figure 2.) The size of the patient determines the size of the cuff selected. There are several cuff sizes. The cuff width should be 20% greater than the diameter of the arm. When a cuff is too narrow, the blood pressure reading is too high; when the cuff is too wide, the reading is too low.
The stethoscope (a listening aid that magnifies sound) is used with manual devices and consists of two earpieces that are connected by tubes that carry the sound to the earpieces from the end piece, which is placed over the artery (see Figure 3.)
PROCEDURE FOR DETERMINING BLOOD PRESSURE WITH A MANUAL DEVICE
It is important that the patient always be in the same position using the same arm. Differences in body position and arm used can make a difference in the reading of 10mm Hg or more. Figure 4 presents a detailed, step-by-step rubric for successfully achieving accurate measurement.
Hypertension should never be diagnosed with only one reading. Blood pressure reading should be taken in a variety of different situations. Some patients will experience “white coat” hypertension.
In January of 2012, a study was released in Lancet regarding the recommendation for taking blood pressure readings in both arms. The study indicated that a systolic number difference of 10-15 mm Hg or more could be an indication of a more serious problem such as narrowing arteries, decreased blood flow to the brain, and a significantly increased chance of heart attack and stroke. Should the dental professional receive such readings, they should take the blood pressure readings again after approximately 5-10 minutes. If the readings received are still inconsistent between the patient’s arms, the patient should be referred to their physician for a blood pressure work up.
PROCEDURE FOR DETERMINING BLOOD PRESSURE WITH AN AUTOMATIC DEVICE
Preparation of the patient is the same when using an automatic blood pressure device. However, the manufacturer’s instructions for using an automatic blood pressure device can be different (Figure 5). Read the manufacturer’s instructions carefully before using the device.
LIFESTYLE MODIFICATION RECOMMENDATIONS FOR PATIENTS
Time restraints at dental appointments prevent in-depth counseling for patients with high blood pressure readings. Instead, it is recommended that you provide information from professional websites, such as the American Heart Association. Their Nutrition Center link provides health goals such as: not smoking, maintaining a healthy weight, engaging in regular physical activity, eating a healthy diet, managing blood pressure, monitoring cholesterol, and keeping blood sugar (glucose) at healthy levels.
SUMMARY
According to the Centers for Disease Control (CDC), hypertension affects approximately one in three Americans. Research studies have shown that people with normal blood pressure readings between the ages of 55 and 65 still have an 80-90% risk of developing hypertension by the age of 80. With patients living longer, blood pressure should be monitored and recorded on a regular basis in the dental practice. The information in this course teaches the dental health professional to be aware of the causes of hypertension and how to determine and assess identifiable causes. A good understanding of the terms systolic, diastolic and pulse pressure along with knowledge of the various blood pressure categories and the factors that influence blood pressure are important. This course provides you with the appropriate method of taking a blood pressure and how to determine the recommendations for follow-up and lifestyle modifications for patient treatment.
REFERENCES
1. Malamed SF. Medical Emergencies in the Dental Office, Sixth Edition. Mosby Publishing, 2007.
2. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) U.S. Department of Health and Human Services. National 3. Institutes of Health. http://hyper.ahajournals.org/cgi/content/full/42/6/1206#FIG18 [Online] February 2005.
4. Wilkins EM. Clinical Practice of the Dental Hygienist, 10th Edition. Lippincott Williams & Wilkins. 2009.
5. Glick M. The New Blood Pressure Guidelines. JADA 2004; 135(5):585-6
6. American Heart Association www.heart.org [Online] November, 2011.
7. Centers for Disease Control and Prevention -http://www.cdc.gov/bloodpressure/facts.htm
8. Consumer Reports. Sept 2008;47-9.
9. National Heart Lung and Blood Institute http://www.nhlbi.nih.gov