You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
The ADAA has an obligation to disseminate knowledge in the field of dentistry. Sponsorship of a continuing education program by the ADAA does not necessarily imply endorsement of a particular philosophy, product, or technique.
We know that a patient's oral health and their overall health are both interrelated. Many medical conditions have oral manifestations that often are the first indicators of a systemic disease. There are also medical conditions that can have detrimental effects on dental treatments.
With these facts in mind, it is apparent that a patient's health history is "the" most important document in a dental practice. The medical history is an assessment of the patient's current health status and can be used to evaluate or identify any current conditions that may alter the treatment plan. Health histories are also important in identifying any patients with infectious diseases, such as tuberculosis, that can pose serious hazards to the dental team and other patients in a dental practice.
It is the legal responsibility of a dentist to obtain a health history from every patient that s/he treats, in order to make informed treatment decisions. Dental assistants are often assigned the task of obtaining this information from patients, are often the first member of the dental team to have contact with patients and many times assist patients in completing their health history forms. Therefore, it is vitally important for assistants to understand the many facets of a comprehensive health history.
Purpose of the Health History
The primary purpose of a patient's health history is to attempt to find out as much about each patient as possible, so that the dental practice can treat the patient safely and knowledgeably. Members of the dental team need to know any and all information about a patient's current health status, as well as any information about past medical and dental treatment; since all these factors will affect treatment, information regarding family history is also helpful to the dental team. Certain health and oral conditions are hereditary in nature and can aid the dentist in diagnosis and troubleshooting.
New patients should complete a form or set of forms that give the dental practice personal information about them, as well as all the previously mentioned dental and medical information. In addition, returning patients should be asked to update this information at each visit. The registration and health history are legal documents, as part of the treatment record for each patient. These documents can be subpoenaed in court cases, such as a malpractice suit, or when disciplinary action is taken against a dental professional by a regulatory board. Because these documents can be used as legal evidence, they must be thorough, accurate and legible.
Under the Health Insurance Portability and Accountability Act of 1996 (HIPAA), these records are also considered Protected Health Information (PHI) and dental practices must take federally mandated steps to protect the privacy of this information. The information may be used in conjunction with treatment of the patient, payment from insurance plans, and the general operation of the dental practice, such as administrative recordkeeping, which is defined by HIPAA as TPO, with a general consent from the patient. If the PHI is to be used for something other than TPO, such as marketing purposes, such as a list of patients that is sold to a company that wishes to mail information about medications or oral care devices, patients' specific written consent must be given for the release of this information. An excellent resource for information regarding HIPAA and compliance requirement for dental practices is the ADA HIPAA Compliance Manual, available from the American Dental Association.
Aside from the legal and recordkeeping aspect of the health history, this document serves as a bridge of communication between the patient's medical health care provider and the dentist. When a patient completes a health history form, either as a new patient, or as a returning patient, emphasis is placed on identifying any conditions that may affect that patient's current dental health, overall health and ability to receive dental care at the time. If the patient indicates certain medical problems, such as a heart condition, the dental team will ask certain questions of the patient and the treating physician to assess the appropriateness of proceeding with treatment and determine if any special precautions must be taken. This information assists the dental team in preventing medical emergencies during treatment. In addition, undiagnosed conditions may be detected as a result of completing and reviewing the health history. For example, a patient who feels healthy may have high blood pressure and not be aware of it. Completing or updating a comprehensive health history on each patient, including checking blood pressure, may identify patients who need medical intervention to treat their condition.
Written documentation of the health history places emphasis on compiling this information. Many patients would not think to tell their dentist about medical conditions, because many of them do not realize that their oral health and general health are interrelated. It then becomes a critical task for every dental assistant to educate patients as to the importance of completing their health history form and providing their dentist with accurate and up-to-date information. This can be accomplished by explaining to patients about the oral manifestations of many diseases, such as diabetes or malnutrition. The dental assistant can also explain to patients that taking certain medications will have effects on the oral cavity, such as decreased saliva or xerostomia (dry mouth.) When patients understand why the information is so important, they may be less resistant to disclosing it to the dental team.
Legal Requirements for Treatment
Legal Consent
When new patients complete a health history or returning patients update an existing history form, it is important to make certain that the patient is of legal age to complete and sign the form. In most states, children under the age of 18 are considered minors. As such, these patients, and patients who are mentally incompetent, must have a parent or legal guardian complete and sign their form for them. Since minor patients are sometimes "dropped off" at the dental office, and the parent does not stay for the appointment, the dental assistant or team member who schedules the appointment or greets the patient must emphasize to the parent and/or patient that the health history form must be completed or updated and signed by the parent or guardian.
Disclosure/Disclaimer
At the end of the health history written questionnaire the patient should be required to sign a statement that serves as a disclosure that the information is complete and accurate and also a disclaimer that the patient does not hold the dentist or other team members responsible for any errors or omission of information they may have made in completing their form. A sample statement is illustrated in Figure 1.
Informed Consent
Before a dental professional performs any type of diagnostic or treatment procedures on a patient, that patient must give their consent. Informed consent, as it is called, involves gaining the patient's permission to proceed with treatment and also explaining to the patient all the facts, risks involved and any alternatives to the proposed procedure. Informed consent also includes informing the patient of the risks of not having a procedure performed. For example, patients who refuse a referral to a specialist for treatment of their periodontal disease must be informed of the risk of losing their teeth due to the disease.
In many cases, informed consent is implied. In other words, the fact that a patient makes an appointment and allows a dentist, assistant, or hygienist to treat him/her, implies that they gave consent for treatment. Attorneys and risk management specialists, however, recommend that informed consent be in written form (Figure 2). This consent form can be attached to or incorporated into the health history form. Many times, specialists, such as endodontists, oral surgeons, periodontists and orthodontists utilize specialized consent forms that detail the possible risks of the specific procedures that they perform. The only instance where a patient or guardian is not legally required to give informed consent, is when the patient is unconscious and in need of emergency treatment. For example, if a patient is having an allergic reaction to latex, you do not need to have them sign a consent form to administer epinephrine to help save them from anaphylaxis and possible death.
Risk Management
Because a health history is a legal document, certain criteria must be met by the dental team members who manage that information. First, all patient records must be completed in ink, to avoid the possibility of alterations to the record. A ballpoint pen is preferred, since many of the felt-tip or roller-ball type pens have water soluble ink, which can wash off the record if liquid is spilled on it. If a mistake is made on the form, have the patient cross out the incorrect information with a single line and initial it. The correct information can be entered just above or below where the incorrect information was written. Correction fluid or tape should never be used on any patient records. If information is transferred from a form completed by the patient to a computerized patient record, always retain the paper copy completed and signed by the patient or guardian.
Some dental practices prefer to send out health history and patient information forms to new patients by sending them an email or directing them to the office's website prior to their appointments, to save time on the day of the appointment. This is an excellent means of managing the appointment time, except if the patients lose or forget to bring the forms with them to their appointment. Sending a stamped, self-addressed envelope along with the forms and asking the patient to mail them back to the office could alleviate that problem, provided that there is enough time for the forms to reach the patient and be returned to the office prior to the patient's appointment.
It is common for new patients to be scheduled for preventive or cleaning appointments at their first visit to a dental practice. If new patients are scheduled for treatment appointments at their first visit, the business assistant or scheduling coordinator must ask some preliminary health history questions prior to receiving the form completed by the patient. In particular, the practice needs to know whether or not that patient needs antibiotic prophylaxis. The current guidelines from the American Heart Association for prevention of bacterial endocarditis should be followed. (Appendix A)
Confidentiality and Privacy. Doctor-patient privilege requires a dentist to hold in strictest confidence any information disclosed by a patient for purposes of treatment. Therefore, all information contained in the patient's record, including the health history, is confidential information to be used only in relationship to the patient's treatment. Patient records must be stored in a secure area that is accessible only to members of the dental team. No information about the patient's medical or dental conditions should be indicated on the outside of the patient's record (file folder). Although it is a common practice to indicate allergies or the need for antibiotic prophylaxis on a patient's file folder, this practice is a violation of patient confidentiality. An alert in the patient's electronic record may be placed, but, again, nothing specific, such as "allergic to penicillin" should be indicated. The dental assistant must read the patient's medical history. This is especially important with regard to transmissible diseases due to the high degree of sensitivity of the information.
If a dental practice is contacted by another health care provider (dentist or physician) for information related to confidential patient information, it is best to have that request confirmed in writing and have the patient sign a "release of information" statement, authorizing the dentist to disclose the information. The exceptions to the doctor-patient privilege law are cases in which the public welfare is in jeopardy. Such cases would be infectious disease (tuberculosis or hepatitis), which may be reportable to the public health department; or child abuse or neglect, which is reportable to law enforcement authorities.
Patients can be reluctant to disclose information about themselves, out of fear of their confidentiality being violated. These patients require the sincere reassurances of all members of the dental team that their privacy will not be invaded and information about them will not be disclosed inappropriately.
Title II of HIPAA sets forth specific requirements for protecting the privacy of the patient's information disclosed on the health history. A dental practice that is a covered entity must have a written privacy policy, which must be given to patients, and explains to patients that the dental practice will not disclose the PHI for any uses other than TPO without the patient's written consent.
Legal Ownership of Patient Records. A patient's records, including the health history and radiographs, are the legal property of the treating dentist. Many patients, however, believe that the records belong to them. According to statutes in nearly half the states in the U.S., patients have a right to review their records and to photocopy their records. Patients also have the right to request that copies of their records (including radiographs) be sent to a new dentist or to a specialist for treatment or a second opinion. The state attorney general's office in each state should be contacted to become familiar with that state's laws concerning access to medical records. Original copies of patient records, especially health histories and radiographs should not leave the dental practice. If radiographs are required for submission of insurance claims, make copies using duplicating film, or use double-film packets when exposing radiographs on patients. In some cases, digital radiographs may be submitted.
Under HIPAA, patients have additional rights to review their records and request corrections or clarifications of the information in those records. Again, additional information regarding HIPAA requirements may be obtained from the ADA HIPAA Compliance Manual.
Techniques for Obtaining a Health History
Written Questionnaire
Since the health history is a legal document, be certain to instruct the patient to complete the form in ink, and to print. This will help prevent problems in reading the information, if the patient's handwriting is illegible. It is preferable to print these instructions at the top of the health history form, to save having to write out or verbally give these instructions each time a form is to be completed.
When designing or updating a questionnaire, it is advisable to use at least a 12 point type font, which is easier for most patients to read. Selecting a serif font will also make the information easier to read. Some dental practices attempt to keep the health history on one side of one 8 1⁄2" X 11" sheet of paper, by using a small font and eliminating some important information. It is advisable to be as comprehensive as possible, using as many pages as necessary. If patients hesitate, because of the length of the form, the dental team members should explain the importance of the information and inform the patients of the need to have a complete picture or summary of their health status. Offering to help patients record the information sometimes alleviates this reluctance.
If the office is computerized and the patient can be questioned in a private consultation or treatment area, information about the health history can be asked and directly entered into the computer database. The dental professional will then transcribe all information into the patient's electronic chart. However, remember to have the patient sign a printed copy of the form, or, some programs can have the patient sign the document.
Oral Interview
Once the health history form is completed, it should be reviewed orally with the patient by the assistant, hygienist or dentist to clarify the accuracy of the information. Several very important questions should always be asked of patients, who may not remember or not consider the information important enough to list on their health history form:
1. What medications are you taking? (Both prescription and over the counter, as well as nutritional supplements)
2. Have you been hospitalized for any reason within the last 6 months?
3. Are you currently under a physician's care? If yes, then for what reason?
This information should be highlighted on the health history form for possible consultation with a physician prior to the patient receiving any dental treatment. The section on "Classification of Patient's Current Status" gives specific information about conditions for which a physician should be consulted prior to treatment. Keep in mind, however, that some patients may not disclose all the necessary information to you on the health history form. Some information is very sensitive, for example, disclosing one's HIV status or current treatment for a sexually transmitted disease (STD), like syphilis or gonorrhea. Therefore, some patients may not want a dentist to know this information, for fear of this information being disclosed to persons outside of the dental practice. For this reason, a health history cannot be relied on as an indicator of the level of precautions that should be taken for infection control procedures. The theory of "Standard Precautions" states that all persons should be treated as if they are potentially infectious for bloodborne transmitted diseases, regardless of their medical history.
Visual Assessment
In addition to verbally reviewing the patient's written information, dental team members should also be performing a visual assessment of each patient. Does the patient appear healthy? Does the patient exhibit signs of exertion when walking from the reception room to an operatory? Is the patient short of breath/breathing hard? Does the patient have any asymmetries of the head/neck or the rest of the body? Can you see the patient's fingernails and nail beds? Do they appear pink, or have a bluish tint? Are the whites of the patient's eyes yellow instead of white? Does the patient have trouble hearing or speaking? Does the patient have problems with manual dexterity? Does the patient have trouble concentrating? As you might guess, all these physical signs have some relationship to systemic conditions, which can affect the patient's ability to be treated safely. These conditions may also be related to the patient's current oral health status. For example, a patient with limited manual dexterity will no doubt have trouble with brushing and flossing. Patients who get very short of breath walking short distances may have some type of uncontrolled cardiovascular or lung disease, such as chronic obstructive pulmonary disease (COPD).
Always remember there are three components to obtaining a patient's health history - written questionnaire; oral interview; visual assessment.
Recording Vital Signs
Once the dental team member has reviewed the written health history, completed an oral interview and visual assessment of the patient, each patient's vital signs should be recorded. As a rule, each new patient's blood pressure, pulse and respiration should be checked and recorded on his/her health history form. Adult patients should be checked at each return visit. Many styles of blood pressure devices are available, with automatically inflating cuffs and digital recorders/printers to make this task simple and fast for the dental team. Be aware, however, that some older blood pressure cuffs contain natural rubber latex (NRL) which could cause a sensitivity reaction for latex allergic patients. NRL cuffs should be replaced with a newer, latex-free cuff that will not pose a risk of allergic reactions.
Communication Skills
Health care literacy has become an issue when obtaining record information. Quite often, a patient may not understand the medical or dental conditions you are speaking of and may need extra time and help to understand the concepts and terminology. A patient may not even be aware that their condition could be considered a disease that needs special consideration while receiving dental treatment. It is the dental team member's responsibility to make sure the patient understands the treatment prescribed before obtained consent for themselves or children.
Obtaining personal information from patients, especially for a health history, requires excellent communication skills. Patients should feel 11 comfortable that the dental team member interviewing them is objective, non-judgmental and sensitive to their needs. The dental assistant or other team member should make eye contact with the patient when speaking and especially when asking questions of the patient. If patients disclose sensitive information, such as HIV status, reassure the patient that this information will be held in the strictest confidence and utilized only in relationship to their dental treatment. Be especially careful not to talk about patients within earshot of other people or patients. Not only is this breaking the confidentiality of the patient, it is not reassuring to patients that you do treat their disclosures confidentially.
It is important to obtain information on all medicines or drugs the patient may be taking at the time of the appointment. Patients must know that any drug, whether taken legally or illegally can affect the dental treatment and recovery times. Drug toxicity or overdose can occur if the patient is not truthful in disclosing all medications to the dental team.
The dental assistant or other team member must also be cognizant of their non-verbal communication with patients. Even though the assistant may not verbally indicate their surprise or distaste at some information that is disclosed, it may be obvious in their facial expressions. It sometimes takes practice to become proficient at staying expressionless and non-judgmental, but it is well worth the effort and could greatly enhance a patient's willingness to disclose all information about his/her health status.
Components of a Comprehensive Health History
Personal Information
There are two classifications of information contained on a health history: personal and medical information. The personal information includes the following: patient's name, address, home phone number, date of birth, current age and gender. For adults, the personal information also includes place of employment, business address and phone number, social security number, spouse's name, birth date and social security number, insurance information (carrier, group number, policy number) and the name of a close relative not living with the patient (in case of emergency). For minors, the information should also include the name of the patient's parent or legal guardian and that person's insurance information and a telephone number at which they can be reached in an emergency. The name of the patient's primary care physician should also be listed. In the case of patients with specific medical conditions, the name of the specialist(s) treating them should be listed. If applicable, the name of the patient's previous dentist should be listed, in order for copies of the patient's previous treatment records and/or radiographs to be requested.
Medical Information
The medical information necessary on a health history form will be the lengthiest and most time-consuming for the patient and dental team to complete. It should include the patient's past history including, for example, whether they have had a previous heart attack; their family history (does anyone in their family have cardiovascular disease?); and a list of all medications the patient is currently taking, including over the counter (OTC) medications, like antihistamines, antacids or nutritional supplements. Recent surgeries and treatments such as chemotherapy or radiation should be noted as the patient may be immuno-compromised and unable to receive treatment. The last component of the medical history is a review of all the body systems, to determine if there are any conditions that may affect, modify or delay treatment. Table 1 is an example of a review of the body systems. See Appendix B for an example of a Medical Questionnaire.
Dental Information
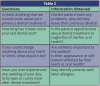
Past History. The health history should contain questions regarding the patient's past dental experiences. Table 2 lists some suggested questions to ask patients about their past dental history. If the patient has indicated who his/her previous dentist was, this information may be verified by contacting that dentist.
Chief Complaint. In order to assess the patient's understanding of his/her oral health and also to determine the patient's expectations, it is important to ask the patient what his/her chief complaint is. In other words, why have they come to the dental office? Does the patient have pain, swelling, bleeding, sensitivity to hot, cold or sweets or difficulty biting/chewing? Is the patient concerned with his/her appearance? If the patient is in pain, it is important to attempt to diagnose the source of the pain and to attempt to resolve the problem, or the patient will feel that his/her needs are not being met and may not remain as a patient in the practice.
Current Conditions. Identification of the patient's chief complaint, along with a clinical oral examination will identify the patient's current conditions. The oral examination should consist of a visual and digital examination of the mouth, head and neck, a radiographic survey, complete charting of teeth and supporting structures, including a periodontal chart. Current conditions should be recorded on the treatment record, as well as entering a summary description on the health history, including classification of existing restorations and teeth (e.g. rampant caries or marginal breakdown on existing restorations) and the periodontium (e.g. moderate gingival inflammation, bleeding on probing). Keep in mind that HIPAA considers the above information to be Protected Health Information (PHI).
Classification of Patient's Current Status
A simple classification system for identifying a patient's health status is illustrated in Table 3. This classification system is based on the patient's medical history, drug history (medications), physical and clinical examination (vital signs), emotional evaluation, medical consultation and personal experiences. Patients in ASA Class I can be treated without medical consultation. The dental team should consult with the patient's physician prior to treating patients in ASA Class II and III. And patients in ASA Class IV and V should not receive dental treatment until stabilized and away from life-threatening danger. After thorough review of the health history, each patient should be assigned a classification that is recorded in the treatment record and revised as the patient's status changes. All members of the dental team should be aware of this classification. Specific information about systemic diseases and conditions is listed in the following sections.
Medical Conditions That Affect Dental Treatment
Once all the information has been obtained from the patient's health history, both oral and written questionnaires, the dental team must evaluate the data and determine if any conditions exist that will affect, alter or delay any necessary dental treatment. The following are conditions that will have some effect on dental treatment:
Need for Antibiotic Prophylaxis. The American Heart Association (AHA) guidelines from April, 2007 are those currently used to determine the need for and the protocol for antibiotic prophylaxis. The AHA, in conjunction with the American Medical Association and the American Dental Association, reviewed and revised the type of patients that need to be pre-medicated for dental treatment. Each office should consult with the patient's physician if unsure of recommended antibiotic prophylaxis prescriptions.
Syncope. Syncope, or fainting, is the most common emergency in the dental office. Patients should be asked if they have ever experienced a fainting episode in a dental office, or at any time in their life. It is most commonly associated with heavy coughing, orthostatic hypotension, and medication. Syncope can happen to any person at any age but most common with geriatric patients.
Diabetes. There are three types of diabetes: Type I is considered insulin dependent, 5-10% of cases; Type II is when the body does not produce enough insulin and, therefore diet and medication may be regulated, 90-95% of cases; Gestational diabetes occurs during pregnancy and is reversed after delivery. If the patient indicates that they have diabetes, the type must be noted in the history.
Patients with uncontrolled diabetes have low resistance to infection and are prone to periodontal disease. They have poor healing response, including excessive bleeding, and may experience hypoglycemia or hyperglycemia during dental treatment. Patients who are undiagnosed diabetics may report the following symptoms: excessive thirst and hunger, increased urination and in women high birth weight babies.
When reviewing a health history, the following questions should be asked of diabetic patients:
• Is your diabetes well controlled?
• When was the last time your blood glucose was checked?
• Are you currently taking oral anti-diabetic medications or insulin injections?
• When was the last time you ate?
It is advisable to keep sources of sugar on hand for hyper or hypoglycemic episodes. Glucose gel from a pharmacy, granulated sugar or tubes of cake icing can be easily stored and used in the case of an emergency.
When questioning diabetic patients before treatment and you find out they have not eaten or taken their insulin they should be rescheduled. Make sure they understand the importance of these steps to maintain a normal blood sugar level during dental treatment. Additional strategies include keeping appointments short and in the early to mid-morning hours.
Cardiovascular Disease. Patients who state that they have experienced chest pain, shortness of breath, pain that radiates down their neck or arm, have swollen ankles and/or have high blood pressure are at risk for cardiovascular disease. They may or may not have been diagnosed by a physician. If this patient also indicates that they are a smoker and/or are overweight, the risk is increased. It is recommended that a medical consultation or evaluation be obtained for all patients who indicate some type of cardiovascular disease on their health histories. Additionally, medical consultations should also be obtained for patients who are reporting or exhibiting symptoms of cardiovascular disease but have not had a definitive diagnosis. Preventing medical crises during dental treatment is the best method of protecting patients who are medically compromised.
Rheumatic Heart Disease is a result from rheumatic fever and can cause deformities in the heart valves. Some patients will report taking antibiotics on a regular basis. If the patient reports a history of rheumatic fever, the dental practice must consult with the patient's physician to determine the extent of the heart involvement, in particular whether the patient has valvar damage.
Congenital Heart Defects place the patient at high risk for bacterial endocarditis. Again, a statement from a physician is advisable to determine the type of defect and to verify the need for prophylactic antibiotics.
Coronary Artery Disease (CAD) results from atherosclerosis. Patients may report having been diagnosed with angina pectoris or having chest pain after some type of physical activity or stress. These patients may be taking several medications, particularly vasodilators like nitroglycerin; or beta-blockers, such as propranolol. The stress of a dental visit may cause an angina attack, therefore it is important to minimize patient stress, maximize patient comfort and make certain that the patient has his/her medications available, particularly nitroglycerin. In addition, it is recommended that local anesthetic without epinephrine or other vasoconstrictors be used for these patients, to avoid further constriction of the blood vessels. Patients with unstable or uncontrolled angina should wait for at least 30 days after their angina is stabilized to receive dental treatment.
Myocardial Infarction (MI) is more commonly known as a heart attack. Patients who have experienced a recent myocardial infarction should not receive any dental treatment for a minimum of 6 months after the heart attack. Most fatalities from MI occur within 3-4 months after the attack. Stress, like that from dental treatment, soon after the attack could cause a rupture in the area of infarct, leading to further health problems and possible death.
Hypertension is a common condition characterized by high blood pressure. Patients with uncontrolled hypertension are at risk for a stroke (also known as a cerebrovascular accident, CVA), kidney failure, or heart attack. Since stress will increase blood pressure, dental treatment is contraindicated in patients with severe hypertension. Patients presenting with a systolic pressure between 120 to 139 should be advised to monitor their readings for improvement and see their physician for assessment. As a rule, patients with a systolic pressure greater than 160 and/or a diastolic pressure greater than 95 should be referred for medical consultation and treatment and dental treatment should be delayed.
It is relatively common for patients to have undiagnosed hypertension, making it very important for the dental team to monitor patients' vital signs during their dental visits. A patient who reports having frequent dizziness, nosebleeds or headaches may have high blood pressure and may be in need of medical intervention with antihypertensive drugs and/or diuretics.
Heart Failure (HF) was more commonly known as "congestive heart failure" but the American Heart Association has recently renamed and shortened the title to characterize a broader spectrum of the disease. Patients with congestive heart failure typically have swollen ankles and shortness of breath, due to poor circulation and fluids backing up in the lungs. These patients may indicate that they must sleep upright or with several pillows, in which case, placing them in a supine position in a dental chair may cause them acute distress. HF patients are usually taking one or more diuretic medications to remove fluid, as well as digitalis to strengthen their heart contractions. Supplemental oxygen may be needed for these patients and use of nitrous oxide analgesia is contraindicated.
Kidney Disease. Patients with kidney disease have impaired renal function, which results in accumulation of fluid and waste products normally excreted by the kidney. Renal problems often result from uncontrolled or undiagnosed diabetes. These patients may experience poor healing and excessive bleeding. They may be receiving dialysis treatments or may have had a kidney transplant. In either case, the patients may be taking medications, such as anticoagulants or immunosuppressive drugs. Consult with the PDR regarding side effects of the medications and with the patient's physician if there is a need to prescribe drugs for patients whose primary method of excretion or metabolism is the kidney. The impaired function of the kidney may cause toxic levels of the drug to accumulate in the patient's tissues.
Seizure Disorder. Seizure disorder is caused by an electrical disturbance in the brain. Any person can experience a seizure in a stressful situation and approximately half of all seizures are considered idiopathic (without known cause.) Epilepsy is a condition commonly associated with a syndrome of associated seizure types.
When a known epileptic patient is scheduled for treatment, the dental team should determine if the patient has taken his anti-seizure medication. These patients should be scheduled for short appointments, when they are well rested. Shining a bright light in the patient‘s eyes should be avoided, since this can sometimes trigger a seizure.
Patients who are taking oral anticonvulsant medications, such as Dilantin®, may experience gingival hyperplasia. Emphasis must be placed on meticulous home care to prevent serious periodontal problems and the increased need for regular dental visits.
Asthma. Asthma is a chronic respiratory disorder that results in a narrowing of airways. An asthma attack can be triggered in several ways including environmental allergens, medications, or exercise. Patients with asthma may be prone to an attack or episode brought on by the stress of dental treatment. The patient is always instructed to bring his/her medication/inhaler to each appointment. When the health history is reviewed at the beginning of treatment, the patient should have the medication or inhaler readied just in case it is needed.
Chronic Obstructive Pulmonary Disease (COPD). The two most common forms of COPD are emphysema and chronic bronchitis. Emphysema is the irreversible enlargement of the air sacs in the lungs making it hard to expel all oxygen during breathing. Chronic bronchitis is characterized as the irreversible condition of narrowed airways. Like patients with HF, those with either of these types of COPD may not be able to breathe easily in a supine position or after walking certain distances. Patients with COPD may need supplemental oxygen and often carry their own supply with them. However, these patients should not be given high levels of oxygen, since this disease prevents them from metabolizing it. It is important that the COPD patient not receive nitrous oxide during dental treatment due to their impaired breathing.
Infectious Diseases. Hepatitis is characterized as an inflammation of the liver. It is a viral disease that appears in several forms. It is referred to as hepatitis A, B, C, D and E. A newer type of virus, non A-E, has been discovered, but not much is known about it at this time. Hepatitis B and C are transmitted through blood or other body fluids, while hepatitis A and E are usually transmitted indirectly through contaminated food and water. Hepatitis D is a piggyback virus that is linked to hepatitis B. Dental health care workers should be vaccinated against hepatitis B, to reduce their risk of infection when treating patients. There is no vaccine for hepatitis C at this time. We are not able to identify every patient who has a potentially infectious disease, and because many patients are not aware that they had hepatitis, and may be carriers, it is important to remember to practice standard precautions.
If a patient presents for treatment and reports that they are fatigued, nauseous, have a fever, dark urine and/or are jaundiced, they should be referred for medical treatment. When a patient reports a history of hepatitis, consult the PDR and their physician if drugs are prescribed that are metabolized by the liver, since liver function may be impaired.
Tuberculosis (TB) is a bacterial infection that occurs primarily in the lungs, but can occur in other organ systems in the body. It is spread through airborne particles, when an infectious patient coughs, sneezes, talks or sings. TB is most easily spread in small confined spaces where infectious people share the same airspace with others. Because TB is highly infectious and its airborne transmission is difficult to control, the CDC has issued specific guidelines to help protect health care workers when treating patients.
These guidelines state the elective (non-emergency) dental treatment should be postponed for patients who are suspected of having infectious TB or who have been identified as active TB cases. If these patients can be referred for treatment in a facility that is specifically designed to treat TB patients (e.g. a hospital setting), it is acceptable for the dental practice to make this referral and not be liable for discriminatory practices.
In addition to asking patients on their health history if they have had tuberculosis, the patients should also be asked if they have experienced any of the following symptoms: night sweats, unexplained fever and/or weight loss or a prolonged or bloody cough. If a patient has experienced any of these symptoms, refer them to a physician for evaluation before proceeding with anything but emergency treatment. If emergency treatment must be performed on a patient suspected of having infectious tuberculosis, the following precautions should be taken:
• Schedule the patient at the end of the day, as the last patient treated.
• All team members present in the treatment room must wear a HEPA or NIOSH N 95 mask.
• High volume evacuation and dental dam isolation should be used to reduce aerosols.
HIV/AIDS is a viral infection that impairs a patient's immune system, making the patient highly susceptible to other infectious diseases. It is transmitted through blood and other body fluids, which puts dental health care workers at some risk of infection from treating patients. Again, the practice of standard precautions must be followed, since many patients will not disclose their HIV status for fear of humiliation or rejection. Remember that information about a patient's HIV status is highly sensitive. The dental team must take every precaution to protect the confidentiality of that patient's health history. HIV or AIDS patients should be treated the same as otherwise healthy patients.
The Americans with Disabilities Act of 1990 protects people with HIV/AIDS infectious and other diseases from discrimination in employment and delivery of all types of services, including health care. Although some dental health care workers are fearful of treating AIDS patients, it is illegal not to accept them into a dental practice or to refer them to another practice, unless the type of treatment is not performed in that practice. For example, if a general dental practice does not perform periodontal surgeries, it is legal to refer HIV/AIDS patients to a periodontist, since non-HIV or AIDS patients are referred as well. However, if only the patients with HIV or AIDS are referred for periodontal surgery, this would be considered discriminatory.
When treating patients with AIDS, who are typically very immune suppressed, the dental team should take extra precautions to protect the patient from opportunistic infections. These may include wearing sterile surgical gloves rather than non-sterile exam gloves, having the patient use pre-treatment rinse of chlorhexidine gluconate or other mouthwash to prevent bacteremia and using only sterile water for irrigation, rather than from the air/water syringe, which may contain some bacterial contamination.
Blood Diseases. Anemia is a deficiency of red blood cells, caused by vitamin or iron deficiency or bone marrow problems. An anemic patient may have problems with slow wound healing and excessive bleeding. They may report feeling weak and fatigued and may appear very pale. If a patient exhibits these symptoms a medical evaluation should be recommended.
Leukemia is a type of blood cancer, where there is an overgrowth of white blood cells. These white blood cells may displace red blood cells, used to transport oxygen in the blood. These patients may exhibit oral signs, often before other symptoms of their disease. These signs typically include excessive gingival irritation in the absence of other causative agents, like heavy plaque or calculus.
Patients with leukemia are very prone to infections, including periodontal infections. In addition, the chemotherapeutic agents used to treat the disease have many side effects, most notably, xerostomia or dry mouth. Consult the treating physician before proceeding with treatment. Also consult the PDR for side effects from medications.
Hemorrhagic disorders are a condition in which patients experience excessive bleeding due to a deficiency of clotting factors in their blood. Commonly known as hemophilia, these patients will bruise very easily and may experience spontaneous, excessive bleeding. In addition, these patients may have received blood transfusions with blood contaminated with HIV and/or hepatitis B or C.
Dental treatment, such as extractions, that may cause bleeding can be risky for these patients. Close monitoring by the physician is necessary. Treatment should be confined to specific areas (e.g. one tooth or quadrant at a time) and transfusion with clotting factors may be necessary prior to treatment. Aspirin containing medications used for pain control must not be prescribed for these patients, since they increase bleeding time.
Allergies. Allergies are specific body responses to foreign substances. An allergic reaction may be localized or limited to a skin rash or hives, or may be systemic and life-threatening, as in anaphylaxis. Many patients will indicate on their health history that they are allergic to environmental agents, such as pollen and dust. Many are also allergic to medications, such as codeine or penicillin. When prescribing medications, it is important to review the health history and orally question patients about drug allergies.
Latex allergies are becoming more common in dental and medical treatment. Repeated exposure to latex or natural rubber latex (NRL) during dental or medical treatment can cause a patient to become allergic. Again, the reaction may be localized, in which the patient's lips become itchy or swollen from contact with latex gloves or dental dam material. Some patients, however, can experience a very serious anaphylactic reaction where their entire body responds when exposed to the allergen. The most serious symptom of anaphylaxis is swelling of the tongue, which closes off the patient's airway. Without medical intervention, particularly without administration of epinephrine, patients can die from anaphylaxis.
A health history should ask questions about any allergies the patient may have, including latex, although some patients may not know that they are latex sensitive. Additional questions on the written questionnaire or oral interview may help to determine if this is the case. Patients should be asked if they have ever experienced stomach cramps, nausea or vomiting after eating bananas, kiwis, water chestnuts or avocados. These foods contain chemicals similar to those in NRL. Also, ask patients if they have ever experienced any itching after handling balloons or after previous visits to the dentist or physician, where the health care providers wore latex gloves.
To safely treat latex allergic patients, all members of the dental team who come in direct contact with the patient should wear non-latex (vinyl or other synthetic material) gloves, and non-latex dental dam should be available if dental dam isolation is used. In addition, the dental team should check all products, such as prophylaxis cups, oxygen masks and other items to determine whether those products contain latex. Latex-free substitutes are available for most products that currently contain latex, and many products are now labeled as "latex free." Latex allergic patients should be scheduled as early as possible in the workday, before a great deal of latex has become airborne in the office from gloves being put on and taken off. Epinephrine auto-injectors, or "epi-pens," should be located in each treatment room, ready to administer immediately to a patient who begins to exhibit signs of an allergic reaction.
Patient Medications can cause a reaction at any time. Some of the most important information gained from a health history is an accurate list of medications that a patient is currently taking, both prescription and over the counter. However, some patients may not know the names of the medications or not think that it is important to list certain ones. For some elderly patients, it may be advisable to ask the patient to bring all their meds with them, so that an accurate list may be documented. Consult the PDR to identify medications, side effects, precautions, and particularly drug interactions and contraindications.
Most medications have some side effects, many of which appear in or affect the oral cavity. Xerostomia, significantly decreased saliva production, is a common side effect of many heart medications and antihistamines used to treat allergies. Patients taking these medications must be advised about the adverse effects that dry mouth can have on their teeth and oral mucosa, especially if their oral hygiene is lacking. In addition, saliva replacements may need to be prescribed. Patients with systemic diseases, such as liver or kidney disease should not be prescribed medications that are metabolized by the liver or excreted by the kidneys.
Reference Guides
Merck Manual. The Merck Manual is a reference book that lists detailed data (signs and symptoms) of systemic diseases. It can assist the dental team members in understanding the process of a disease, precautions that should be taken and possible medications that the patient may be taking. The Merck Manual is also available online at www.merck.com/pubs/manual.
Physicians' Desk Reference. The Physicians' Desk Reference or PDR is a reference that gives information on prescription and some non-prescription drugs. The PDR can be used to identify side effects, precautions and drug interactions. It can also be utilized to identify medication by their size, shape and color; in cases where patients do not know the name of a prescription drug they are taking. The PDR is updated yearly and includes mid-year supplements for the newest prescription drugs. It is available in a hardbound book, on CD-ROM, or online at www.pdr.net.
Release of Medical Information from Physician/HIPAA Privacy Rules
Due to the confidentiality of medical information and the physician-patient relationship, all requests for medical consultation information on patients should be made in writing, with the patient's signature authorizing the release of the information. Figure 3 is a sample release form. In some cases, the release form may be sent to the physician with the patient or through the mail. In other cases, to save time, the form may be sent by fax and returned in this manner. This electronic transmission of protected health information is covered by HIPAA and the dental practice must have a one-time signed consent form signed by the patient for the transmission of this information, in addition to the release that must be signed for the physician to release the information to the dental practice.
Updating the Health History
Each time a patient visits the dental office for treatment, the health history should be updated. If it has been a relatively short time since the patient was seen in the office (weeks or months) the health history can be updated verbally, by asking if there have been any changes and if the patient is taking any new or different medications. Once this information is obtained, the patient must initial and date the health history form, to validate the updated information. The dental team member who updates the information should also initial the updates. A common method for facilitating this update is to create a section on the health history form with blank lines for initials and dates (Figure 4).
If it has been several years since a patient has been treated in the office, it is recommended that the patient complete a new health history form, since there may be many changes, not only to medical information, but to personal information as well. When the patient completes a new questionnaire, it should be attached to the old form. The outdated or "old" form should never be thrown away or destroyed.
Summary
The health history is a very important component of the patient record. By using a comprehensive form, the office can properly treat their patient and also prevent possible medical emergencies from occurring in the dental office. The information contained in this course should allow the dental professional to design a health history questionnaire or revise an existing questionnaire to be more comprehensive. This course provides basic information for the professional to remember when interviewing patients and in minimizing the risks associated with treating patients, especially those with medical conditions and assist in providing safe treatment to all patients in a dental practice.
Glossary
Age of consent - In most states, 18 years of age, the age at which a person is considered an adult and can enter into contracts and agree to medical treatment.
Anaphylaxis - An acute, systemic allergic reaction that occurs when a sensitized person is again exposed to the sensitizing agent.
Angioedema - A manifestation of anaphylaxis, characterized by hive-like skin eruptions that are large and swollen both in the dermis or top layer of the skin and the subcutaneous structures.
Antibiotic Prophylaxis - A regimen of antibiotics that is given prior to certain procedures including some dental procedures, to patients who are at risk for bacterial endocarditis.
Atherosclerosis - A condition in which the walls of the artery become thickened, obstructed and/or lose their elasticity.
Bacteremia - Sometimes called septicemia, the invasion of the circulation (blood) by bacteria.
Bacterial Endocarditis - Sometimes referred to as subacute bacterial endocarditis (SBE), a microbial infection of the inner lining of the heart.
Cardiovascular Disease - A collection of diseases that involve the heart and circulatory system.
Cerebrovascular Accident (CVA) - Commonly referred to as a stroke, a disruption of blood flow in the brain or a hemorrhage in the brain.
Chemotherapeutic Agents - Drugs or chemicals used to treat specific diseases, often cancers.
Chlorhexidine Gluconate - An antimicrobial or antiseptic agent used in hand scrubs and mouth rinses.
Chronic Obstructive Pulmonary Disease (COPD) - A term used to describe diseases of the small airways or bronchioles in the lungs, resulting in obstruction, narrowing or collapse.
Congenital Heart Defects - Anomalies that are present in the heart at birth, may involve heart valves, chambers or the walls of the heart (e.g. a hole in the heart).
Coronary Artery Disease (CAD) - A disease that disrupts the flow of blood in the vessels surrounding the heart, typically with a blockage of the artery.
Dialysis - A treatment for patients with kidney failure, in which the blood is circulated through a machine that filters out the toxins normally removed by the kidney.
Diastolic Pressure - The bottom number of blood pressure ration (i.e. 120/80), which measures the pressure in the blood vessel during ventricular relaxation, when the heart is at rest.
Digital Examination - Examination performed with the fingers, by feeling or palpating.
Disclaimer - On a patient's health history means that the patient should sign a statement that he has completed the information to the best of his ability and will hold the dentist harmless if he (the patient) was not truthful and/or accurate on the questionnaire.
Disclosure - With regard to dental treatment means that a dentist must inform patients of all aspects of treatment, benefits, risks and alternatives (as in informed consent).
Discrimination - Denying a person access to services based on race, color, sex, national origin, age, size or any other characteristic, including HIV/AIDS status.
Emphysema - Destruction of the alveolar walls of the lungs, resulting from chronic irritation, such as cigarette smoking.
Epinephrine - Also known as adrenaline, a hormone secreted by the adrenal gland which causes vasodilation of the blood vessels of skeletal muscles, vasoconstriction of the arterioles of the skin and mucous membranes, relaxation of the bronchiolar smooth muscles and increased heart rate. Epinephrine is used as a vasoconstrictor in local anesthetics to prolong their effect. It is also used in treating an allergic reaction to help in relaxing the bronchioles to allow the patient to continue breathing.
Hemorrhagic Disorders - Diseases of the blood in which spontaneous or excessive bleeding occurs.
Heart Failure (HF) - Once more commonly known as "congestive heart failure," HF is a cardio-vascular disease characterized by cardiac output that is insufficient to meet the body's needs, even at rest.
HEPA Mask - High Efficiency Particulate Air, a mask able to filter out very minute particles from the air. It is a special mask designed for use when working with patients with airborne infectious diseases, such as tuberculosis.
HIPAA - Health Insurance Portability and Accountability Act of 1996, a federal law that allows for greater access to health care insurance coverage and mandates that certain procedures be followed by health care providers to protect the privacy of patients' health information.
Hyperglycemia - An increase in the concentration of sugar/glucose in the blood, a feature of diabetes.
Hypertension - Abnormal elevation of the systolic or diastolic arterial pressure.
Hypoglycemia - A very low concentration of sugar/glucose in the blood, usually less than 40mg/100ml of blood. Symptoms include nervousness, hunger, weakness, dizziness and fainting.
Informed Consent - A written or implied acceptance of proposed treatment by a physician; includes informing patients about the treatment's associated risks, alternative treatments and consequences of not having a specific treatment.
Intramuscular - Giving an injection into the skeletal muscle (e.g. upper arm or buttock).
Intravenous - Injecting medication directly into a vein, which provides much faster action of the medication.
Latex/Natural Rubber Latex (NRL) - A milky white fluid that is produced by some seed plants that is the basis for rubber and is the major component of latex gloves.
Myocardial Infarction (MI) - Necrosis or death of myocardial tissue, due to disruption of blood/oxygen flow to the tissues of the heart.
NIOSH N95 Mask - sometimes referred to as a particulate respirator, a mask that is able to filter out very minute particles from the air. It is a special mask designed for use when working with patients with airborne infectious diseases, such as tuberculosis.
Orthostatic Hypotension - a sudden drop in blood pressure caused by a change in body position; for instance, standing too quickly after laying prone for dental treatment.
Palpitation - The perception of the heart action by the patient, a heightened sense of awareness.
Paralysis - Loss of movement and/or sensation due to injury or disruption of the central nervous system.
Protected Health Information (PHI) - Information about patient's health that may not be released without the patient's specific written consent for any use other than treatment, payment or operation of the dental practice.
Rheumatic Heart Disease - Results from rheumatic fever and causes rigidity or deformity of the heart valves.
Risk management - Procedures and protocols designed to prevent errors in the treatment of patients, including recordkeeping and documentation.
Seizure - A disorder of brain or cerebral function which causes altered consciousness, convulsions and/or loss of motor control.
Standard Precautions - A protocol for infection control procedures for health care workers in which the health care workers must assume that every patient is a potential carrier of infectious disease and therefore must wear personal protective equipment and sterilize or disinfect items used in the treatment of that patient, regardless of his or her medical history.
Systolic Pressure - The top number of blood pressure ration (i.e. 120/80), which measures the pressure in the blood vessel at the point of ventricular contraction of the heart.
TPO - Treatment, payment and operations - defined by HIPAA as an appropriate use of protected health information (PHI) with a general consent from a patient.
Urticaria - Hives, local wheals (round, raised areas) and redness of the skin, typically seen in an allergic reaction.
Xerostomia - An absence of or marked decrease in the production and flow of saliva, which may be the result of medication, stress or radiation therapy to the head and neck.
References
American Dental Association, "HIPAA Compliance Manual," 2002.
American Dental Association, "Prevention of Infective Endocarditis: Guidelines from the American Heart Association," Journal of the American Dental Association (JADA), June 2007, vol. 138, pages 739-760.
American Dental Association, "Advisory Statement, Antibiotic Prophylaxis for Dental Patients with Total Joint Replacements," Journal of the American Dental Association (JADA), July 1997, vol. 128, pages 1004 - 1007.
Centers for Disease Control and Prevention, "Guidelines for Preventing Tuberculosis Transmission in Health Care Facilities," 1994.
Dajani, MD, Adnan, et al., "Prevention of Bacterial Endocarditis, Recommendations of the American Heart Association," Journal of the American Medical Association (JAMA), June 11, 1997, vol. 277, no. 22, pages 1794 - 1801.
Grimes, E. B.: "Medical Emergencies; Essentials for the Dental Professionals." Pearson/Prentice Hall. Upper Saddle River, NJ, 2009.
Kleinman, D.V. and Horowitz, A.M. "Oral Health Literacy," Woman Dentist Journal, July 2007, pgs 24-28.
Little, J.W. and Falace, D.A.; "Dental Management of the Medically Compromised Patient," 6th Edition, Mosby Inc., 2002.
Malamed, S.F.; "Handbook of Medical Emergencies in the Dental Office," 5th Edition, Year Book Medical Publishing, 2000. Medical Economics, "Physicians Desk Reference - PDR," Medical Economics.
Phinney, D.; Halstead, J.; Dofka, C.; "Delmar's Dental Assisting: A Comprehensive Approach," Delmar Learning, 1st Edition, 1999.
Berkow, R.; Editor in Chief, "The Merck Manual of Diagnosis and Therapy," 17th Edition, Merck & Company, Inc., 17th Edition, 1999.
Rule, DDS, MS, James T.; and Veatch, PhD, Robert M.; "Ethical Questions in Dentistry," 1993 Quintessence Publishing Co., Inc.
Bird, D. and Robinson, D; "Torres and Ehrlich Modern Dental Assisting," 7th Edition, W.B. Saunders, 2002.
Tyler, M.T.; Editor, "Clinician's Guide to Treatment of Medically Complex Dental Patients," American Academy of Oral Medicine, 2001.
United States Congress, "Public Law 101-336 Americans with Disabilities Act of 1990," July 26, 1990.
U.S. Department of Health and Human Services, "Health Insurance Portability and Accountability Act of 1996."
Woodall, RDH, MA, PhD, Irene R.; "Comprehensive Dental Hygiene Care," Fourth Edition, 1993 Mosby-Year Book, Inc.
About the Authors
Mary Govoni, CDA, RDA, RDH, MBA
Mary Govoni is a certified and registered dental assistant and a dental hygienist. She has been involved in dentistry for over 30 years as a chairside assistant, office administrator, clinical hygienist, educator and consultant. She is a past president of the American Dental Assistants Association, a member of the Office Safety and Asepsis Procedures Research Foundation, the Academy of Dental Management Consultants, the National Speakers Association and served on the Michigan Board of Dentistry. Mary is President of Clinical Dynamics, providing in-office consulting and seminars for dental teams throughout the country.