You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
OVERVIEW OF OCCUPATIONAL DISEASES OF DENTAL MEDICINE
When one considers the types of infections that are of major concern to dental professionals, it becomes readily apparent that a variety of bacterial, viral, and other microbial agents are associated with many acute and chronic conditions. One group of these disease states, viral hepatitis, can have a short- or long-term incubation interval, depending on the etiologic agent involved. The possibility of prolonged symptomatic and asymptomatic sequelae to primary infection also exists. The variability of these features has made it difficult to trace accurately the sources of suspected hepatitis outbreaks; however, as knowledge has increased about the viral etiologies and sensitive diagnostic assays have been developed, we have been able to find more answers to clinically important questions.
HEPATITIS
Definition and Symptomatology
The most straightforward definition of hepatitis is that the condition represents an inflammation of the liver. This does not differentiate between hepatitis induced by chemical agents or as a sequela to viral infection. It is thus of initial importance for dental professionals to remember that a patient history of hepatitis does not automatically signify viral hepatitis. This may be difficult to comprehend initially, because hepatitis conditions in general are similarly divided into prodromal, icteric, and convalescent phases, regardless of the etiologic agents.
During the initial prodromal stage, non-specific respiratory and/or gastrointestinal symptoms
can arise. Patients may complain of a variety of symptoms, including malaise, right upper quadrant abdominal pain, loss of appetite, headaches, nausea, and flu-like respiratory symptoms. Fever may be present but is usually low-grade. Just before the definitive diagnosis of hepatitis B, for example, a highly suggestive prodromal series of symptoms can become manifest: arthritis and widespread maculopapular skin rashes. It is important to note that all or none of these manifestations may occur, as many cases of hepatitis are subclinical and therefore asymptomatic.
The subsequent icteric phase is characterized by the appearance of jaundice and dark, often foamy urine. Of the two, darkened urine is generally noted most frequently by patients. A change in stool color also may occur during this period, in some instances lightening to a grayish-white appearance. Symptomatology in the icteric phase is also variable, as evidenced by retrospective studies in which diagnosed patients were asked to recall earlier symptoms. While the clinical sign of jaundice detected either on the skin, sclera, nail beds, or gingiva is generally regarded as the hallmark manifestation of hepatitis, the majority of infections may only result in elevation of certain serum enzymes associated with liver cells (aminotransferase; transaminases). Elevation of these biochemical markers in blood usually occurs a few days prior to or at the time of clinical symptoms. Other physical signs of hepatitis include hepatic tenderness, hepatomegaly and splenomegaly (enlargement of liver and spleen, respectively).
These major symptoms disappear during the convalescent or recovery phase of viral hepatitis. Even in those individuals who recover normally without any long-term, chronic sequelae, feelings of malaise and fatigue may persist for weeks to months. Variations from this generalized picture are described in the discussion of the specific types of viral hepatitis.
Hepatitis A
Hepatitis A virus (HAV) is a small single-stranded RNA virus, which shares some properties with the picornavirus class. It has been shown to exhibit features similar to the enteroviruses. HAV is more resilient to temperature and pH changes than the enteroviruses, however, and is also able to survive in feces and in exudates, and for weeks on inanimate surfaces.
Hepatitis A was formerly known as "infectious hepatitis." This term is no longer considered an acceptable description of the disease. One of the reasons for the change in terminology has to do with the possible false sense of security people may get by thinking that other viral hepatitis syndromes are not infectious.
Transmission of HAV occurs primarily by the fecal-oral route under conditions of overcrowding, poor personal hygiene, and close contact between infected and non-infected persons. HAV infection is most often indirectly transmitted via contaminated water or food, particularly raw or inadequately cooked shellfish. Common-source outbreaks have occurred in child day-care centers and from food handled by infected food industry personnel. Blood-borne transmission of HAV can also occur but is very rare. HAV is maintained in the population through serial propagation. A carrier state has not been demonstrated, nor has HAV been shown to result in chronic hepatitis.
The clinical course of hepatitis A ranges from asymptomatic to severe. Fever is often present during acute hepatitis A, but symptoms may last only two to seven days. Sudden onset of the illness is characteristic of HAV. It is highly contagious during its incubation period (two to six weeks) and the early stage of acute disease. Once symptoms develop, viral concentration and the likelihood of transmission decrease.
Two single-antigen Hepatitis A vaccines are currently licensed in the United States for people aged 2 years and older. A formalin-inactivated vaccine, Havrix® (manufactured by GlaxoSmithKline) became available in 1995. After the initial dose, the second dose is given six to twelve months later. The second vaccine is VAQTA®, also an inactivated vaccine, is manufactured by Merck & Co. After the initial dose, the second dose is given six to eighteen months later. These vaccines have been shown to be highly effective in producing protective antibodies in studies with both adults and children. It is estimated that the vaccine will protect for at least 20 years.
Twinrix®, a combination vaccine was developed in 2001 to protect against both hepatitis A and hepatitis B. Twinrix® [hepatitis A inactivated & hepatitis B (recombinant) vaccine] is indicated for vaccination of persons aged 18 years and older if there is an indication for both hepatitis A and B vaccination. (Table 1)
Persons at increased risk for infection with hepatitis A include:
• Travelers to intermediate and high HAV-endemic countries
• Men who have sex with men
• Illicit drug users
• Persons with chronic liver disease, and those who have received or are waiting for liver transplant
• Persons who work with HAV-infected primates or work with HAV in the laboratory
• Persons who have clotting factor disorders (hemophilia)
Although hepatitis A vaccination is not routinely recommended for all children in the United States, it is recommended for individuals in the risk groups identified above and for children living in counties and states with a higher prevalence of HAV.
Diagnosis of hepatitis A infection is confirmed by the identification of HAV antibodies (anti-HAV) in the serum. Early in the course of the disease, the anti-HAV is of the IgM class of immunoglobulins. These antibodies persist for four to six weeks and are then replaced by antibodies of the IgG class. The latter remain in the serum indefinitely and confer permanent immunity to hepatitis A.
Hepatitis B
Properties of Virus and Morphological Components
Hepatitis (HBV) is a 42 nanometer (nm) DNA virus containing a complex antigenic structure. This virus has been classified as a member of the Hepadnaviruses. It is very specific in its colonization requirements as it infects only humans and some primates. This characteristic has limited the development of routine in vitro cultivation techniques for HBV. The viral structure has had to be delineated by detection and identification of specific serologic markers rather than culture of the virus.
The complete virion of hepatitis B is called the Dane particle. This particle is capable of replication and constitutes the infectious agent. The outer protein coat of the virus, termed hepatitis B surface antigen (HBsAg), is detectable in infected blood and saliva as a surface component of the intact HBV and as freely circulating, noninfectious spherical and tubular forms. These latter particles represent excess HBsAg shed during viral replication. They comprise the major proportion of surface antigen following infection. This important component was the first serologic marker discovered for HBV. It was initially termed the "Australia antigen" or "hepatitis-associated antigen (HAA)" by Blumberg and associates. HBsAg remains the major diagnostic antigen for hepatitis B infection.
Resistance
Scientists have accumulated little information regarding the precise inactivation curves of HBV. However, new methods of testing germicides for efficacy in inactivating HBV using the duck hepatitis virus test (DHVT) have been formally recognized by the Environmental Protection Agency (EPA). The duck hepatitis virus is considered an appropriate surrogate organism for testing efficacy in inactivation of the human hepatitis B virus. In recent years, germicide manufacturers have begun to include claims for inactivation of the hepatitis B virus on label claims. Disinfectants with the ability to destroy M. tuberculosis within a ten-minute exposure (i.e., hospital-level, intermediate disinfectants) also are considered capable of inactivating HBV on surfaces.
Transmission
In the 1980s approximately 260,000 people were infected with the hepatitis B virus in the United States. Since the introduction of the hepatitis B vaccine and improved infection control precautions that number has declined dramatically to an estimated 38,000 total new infections in 2008. There are an estimated 800,000 to 1.4 million people with chronic hepatitis B virus infection in the United States. Globally, approximately 350,000 people are affected and an estimated 620,000 die each year from hepatitis B.
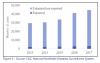
In 2017, a total of 3,409 cases of acute hepatitis B were reported to CDC, for an overall incidence rate of 1.1 cases per 100,000 population (https://www.cdc.gov/hepatitis/hbv/hbvfaq.htm#ref01). After adjusting for under-ascertainment and under-reporting, an estimated 22,200 acute hepatitis B cases occurred in 2017.
The rate of reported acute hepatitis B cases has remained stable over the past decade, with a slight increase occurring in 2017.
The disease can be transmitted via direct or indirect modes of cross-infection. HBV has been detected in blood, saliva, semen, and other body secretions and fluids. The direct transmission of this virus to susceptible individuals by contaminated blood or sexual intercourse has been well documented. Vertical transmission from expectant mothers to their offspring at birth is a common mode of HBV infection. When a pregnant woman is also an HBV carrier, passage of the virus to the fetus is very common, with a high risk of induction of an HBV carrier state in the fetus, chronic hepatitis, and eventually, an increased risk for liver cancer. HBV carried in serum may be spread indirectly through blood transfusions or the administration of blood-derived products.
Of particular concern to dental care providers is the information that indicates that improperly sterilized instruments, needles, and syringes, when contaminated by blood or blood products, can serve as a source of HBV transmission. As little as 2.5 x 10-5 ml of HBV-contaminated blood (versus 1.0 x 10-2 ml with HAV) has been shown to cause disease. Therefore, the use of appropriate methods of sterilization or disposable items should be routine in the practice.
Course of Disease and Diagnosis
Many cases of hepatitis B are not recognized, owing to their asymptomatic or mild course. Approximately 50 to 60 percent of infected individuals develop a subclinical infection. When clinically apparent, the disease often has an insidious onset with nonspecific prodromal symptoms such as malaise, fatigue, and loss of appetite. These symptoms may last for several weeks or up to several months, depending on the extent of HBV infection and the immune status of the host. Anicteric infection (absence of jaundice) is more commonly seen than jaundice and is associated with milder symptoms. Serum transaminase levels indicative of hepatocellular injury may be more than ten times the upper limit of normal values, but are less elevated in milder infections. Symptoms in patients with icteric HBV infection gradually diminish after establishment of jaundice. Full recovery occurs by the end of six months in 90 to 95 percent of patients following acute icteric infection, and by the end of the third or fourth month in 80 percent of the total number of cases.
The development of specific assays for HBV markers has enabled dental health professionals to monitor the course of infection in a quantitative, sensitive manner. Table 2 explains the interpretation of various blood tests available for determining immunity and infectiousness related to the hepatitis B virus.
It is important to note here that the definitive diagnosis of hepatitis B is made by serologically demonstrating the presence of HBsAg. This surface antigen usually is detectable in the blood four to eight weeks after parenteral exposure, but it may appear as early as six days or as late as 24 weeks. HBsAg becomes detectable before clinical symptoms of hepatitis and before any other abnormal lab findings. Serologic levels of HBsAg may peak and actually begin to decline by the time the patient first becomes visibly ill. It is therefore very important to test for the presence of HBsAg as soon as the diagnosis of hepatitis B is suspected. After a variable interval of weeks to months, most patients begin to recover, with HBsAg rapidly becoming undetectable as transaminase enzymes and bilirubin concentrations return to normal. Specific antibody against the core antigen (anti-HBc) appears while HBsAg is still evident. In contrast, synthesized immunoglobulins to HBsAg (anti-HBs) correlate well with the development of protective immunity against HBV.
The significance of anti-HBs in an unvaccinated individual's serum may be summarized as follows:
• Denotes a previous clinical or subclinical infection with HBV
• In most cases means the person has recovered from hepatitis B infection, and is probably immune to reinfection
Hepatitis B Carrier State and Chronic Hepatitis B
Infection with HBV results in a prolonged carrier state in 5 to 10 percent of infected persons. Surprisingly, the carrier condition is more frequently seen following milder anicteric disease. The majority of HBV carriers are asymptomatic and are frequently unaware of having had the disease, but they can transmit HBV via blood, bloody saliva, whole saliva, semen, and other secretions. These individuals continue to produce virus although they appear asymptomatic. The presence of HBsAg is most often used to identify the individual likely to transmit HBV infection. The persistence of hepatitis B antigen (HBeAg) levels is also used as a criterion of high patient infectivity and an increased potential to transmit disease. In addition, the possibility exists
for potential HBV transmission by individuals having HBsAg at undetectable levels but high titers of anti-HBc in the absence of anti-HBs.
Approximately 15-25 percent of HBV carriers have evidence of chronic hepatitis with laboratory or histologic evidence of continued hepatocellular damage. Chronic hepatitis B exists as two morphologic variants: chronic persistent hepatitis and chronic active hepatitis. The former is characterized by inflammatory infiltration and expansion of the portal tracts, minimal fibrosis, and normally appearing parenchymal cells. Chronic active hepatitis is characterized by irregular necrosis of the hepatic parenchymal cells and may gradually progress to cirrhosis. In recent years, treatments with injected interferon and other antivirals have shown some success in eradicating the HBV carrier state. While not universally used, interferon can demonstrate a 35 percent effectiveness in eradicating this chronic, possibly lifelong condition.
Hepatitis C Virus
Introduction
Hepatitis C virus (HCV) is the most common chronic bloodborne infection in the United States. Throughout the 1980s there was an average of 242,000 new infections each year. Since the introduction of reliable blood tests in the early 1990's and subsequent tissue, donor organ and donor blood screening, by 1996 that number had dropped to about 36,000 new cases each year. Most of the estimated 3.9 million Americans infected with HCV are chronic carriers who are at an increased risk for chronic liver disease. Many chronically infected individuals are unaware of their infection and do not have symptoms of clinical illness. In 2017, a total of 3,216 cases of acute hepatitis C were reported to CDC. After adjusting for under-ascertainment and under-reporting, an estimated 44,700 acute hepatitis C cases occurred in 2017.
Transmission and Symptoms
Risk factors that have been associated with transmission of HCV and the following people will be at a higher risk to acquire HCV:
• Recipients of clotting factor concentrates made before 1987
• Recipients of blood transfusions or organ transplants before July 1992
• Current or former injection drug users
• Chronic hemodialysis patients
• Those already infected with HIV, and children born to HCV + mothers
• Health care workers involved in exposures
• Recipients of blood or organs from a donor that has since tested HCV +
Medical and dental procedures and foreign travel have not been implicated in increased risk for transmission. In September 2013, the first documented cases of patient to patient transmission of HCV occurred when an oral surgery office was not following proper infection control protocol for instrument care and sterilization. Although this type of incident is rare in the dental office, it is a soberly example of how important it is to follow standard infection control procotols at all times.
About 75 percent of infected individuals will have no clinical symptoms of HCV. Symptoms that may occur include jaundice, fatigue, dark urine, abdominal pain, loss of appetite, fever, clay-colored stool, joint pain, nausea, and vomiting.
Prevention
For the general population, prevention efforts are targeted at avoidance of high-risk activities such as unprotected sex with multiple partners and the use of shared needles for injecting drugs.
Healthcare workers who have exposure to blood are at risk for infection with any of the bloodborne pathogens. Prevalence of HCV infection among healthcare workers has not been found to be greater than the prevalence among the general population. The average incidence of anti-HCV seroconversion after accidental percutaneous exposure from an HCV-positive source is 1.8% (range: 0%--7%). In contrast to HBV, the epidemiological data for HCV suggest that environmental contamination with blood containing HCV is not a significant risk for transmission in the health-care setting. For these reasons, adherences to standard precautions are considered adequate in controlling the spread of HCV from worker to patient, patient to worker, and patient to patient. No work restrictions are recommended for HCV-infected healthcare workers.
Post-exposure Management
Post exposure protocols for exposures to blood should include considerations for HCV exposure. Source patient testing to determine if exposure to HCV has occurred is an important element of the exposure follow-up. Early identification of infection presents an opportunity for early identification of chronic disease and referral for appropriate treatment. Post exposure follow-up should be conducted by a qualified medical professional that is aware of current recommendations for testing and post exposure prophylaxis medication.
Historically, the drugs most commonly used for hepatitis C treatment are interferon and ribavirin. Interferon is actually a naturally occurring protein that the body makes in response to viruses and bacteria. Unfortunately, when interferon is administered, it usually causes several unpleasant side effects. These side effects may be severe enough to cause patients to stopor refuse treatment. Some side effects of interferon treatment include:
• Fatigue
• Flu-like symptoms, including fever, muscle aches, and headache
• Anxiety
• Depression
• Nausea, vomiting, and diarrhea
In December 2013 Sofosbuvir (Sovaldi®) was approved by the U. S. Food and Drug Administration as the cornerstone for the first non-interferon containing combination treatment for chronic hepatitis C. Although it is very expensive,it can ve a very effective regiment for many hepatitis C patients. No vaccine is currently available for prevention of transmission.
Hepatitis D (Delta Hepatitis)
Hepatitis D originally was called delta hepatitis following its discovery by Rizzetto and colleagues in 1977. As subsequent investigations isolated and characterized the etiologic agent, it became apparent that hepatitis D virus (HDV) was distinctly different from HBV and the other hepatitis viruses. HDV is a defective RNA virus, which is unique in its inability
to accomplish its own replication within infected hepatocytes. This microorganism requires HBV to function as a helper virus by providing a surface coat protein (HBsAg) necessary for synthesis of progeny viruses. In a real sense HDV may be considered a "parasite of HBV," and its epidemiology closely parallels that of HBV.
Outbreaks of HDV have been reported in the U.S., the largest of which occurred in Worchester, Massachusetts. More than 700 cases of hepatitis were diagnosed between 1983-1988 in that area, with more than 65 patients testing positive for HDV. Of the 14 deaths attributed to this outbreak, 11 were HDV- positive. In February of 2009, The National Institutes of Health (NIH) reported that 15 million people worldwide are infected with HDV.
HDV is spread primarily through shared needles. Patients that are known to be HBV positive should be counseled on the prevention of HDV contraction and the increased exposure to HDV when abusing IV drugs and sharing needles.
Infection with HDV occurs via two modalities: 1) simultaneous co-infection with HBV, and 2) superinfection in hepatitis B carriers. The most common outcome of simultaneous HBV and HDV infection is an episode of acute hepatitis followed by recovery from both viral infections. Fulminant hepatitis develops in occasional cases. In HDV superinfection in HBsAg carriers, the dually infected individuals are more likely to have serious, possibly fatal, acute fulminant hepatitis.
Hepatitis E Virus
Hepatitis E virus (HEV) is a major etiologic agent of enterically transmitted non-A, non-B hepatitis worldwide. Clinically, it is most closely associated with hepatitis A in that it is passed through contaminated water and food supplies. As such, it should not be considered an increased risk for occupational transmission in the dental setting. The incubation period following exposure can range from 15-60 days. Virus excretion in the stools appears to continue for about 2 weeks after its first appearance. The symptoms are similar to those for other hepatitis viruses in that the patient may experience abdominal pain, loss of appetite, dark urine, fever, hepatomegaly, jaundice, malaise, nausea, and vomiting. The mortality rate is very low with HEV. No chronic phase is associated with hepatitis E virus, meaning that once a patient recovers, they do not continue to be at risk for subsequent liver disease due to the infection, nor do they continue to pose a transmission threat.
Contaminated drinking water is the most commonly documented vehicle of transmission for HEV, rather than person to person contact. hepatitis resulting from exposure to HEV in the United States has been limited to individuals with recent travel to HEV-endemic areas of the world rather than exposure domestically.
Non A-E Hepatitis
Non-A-E hepatitis, sometimes referred to as hepatitis X, is a disease of the liver that is diagnosed when there is swelling of the liver (hepatitis) but examination and testing does not identify a cause. Symptoms of non-A-E hepatitis may include feeling tired or unwell (malaise), nausea, vomiting, pain in the abdomen, and fever. Non-A-E hepatitis usually goes away on its own, but it can become a chronic condition in a small proportion (12%) of affected individuals. The cause of non-A-E hepatitis is currently unknown.
IMMUNOLOGICAL PREVENTION OF DISEASE
ARTIFICIAL PASSIVE IMMUNITY
Hepatitis B immune globulin (HBIG) has been used in certain defined circumstances. These include: needle-stick or mucous membrane exposures in susceptible individuals with blood from an HBsAg positive individual, and in conjunction with the hepatitis B vaccine for a newborn whose mother either has contracted active hepatitis B during pregnancy or is a chronic HBV carrier. HBIG is prepared from the plasma of individuals known to have circulating anti-HBsAg. This commercial product contains approximately 1 to 2x104 times more of this specific antibody than ISG, and therefore is preferred in the immunoprophylaxis of hepatitis B.
ARTIFICIAL ACTIVE IMMUNITY-HEPATITIS B VACCINES
Plasma-derived Vaccines
The search for a successful vaccine against hepatitis B began in the late 1960s. Krugman and co-workers demonstrated that infective serum (strain MS-2), containing HBV diluted 1:10 in distilled water and heated to 98°C for one minute, prevented or modified the disease in approximately 70 percent of susceptible individuals. The MS-2 serum contained large quantities of hepatitis B surface antigen (HBsAg). Much of the subsequent work focused on the extraction and purification of this non-infectious, viral coat protein for use as the vaccine preparation. This effort was fostered by the observation that replication of the hepatitis B virus in infected individuals was not nearly as efficient as the large amounts of excess coat proteins synthesized and passed into the circulation. As patients recovered from viral infection, antibodies to this antigen (anti-HBs) appeared and were protective against recurrent viral attack.
Accumulated evidence also indicated that these HBsAg forms are present in high concentration in carriers of hepatitis B. Thus, carriers with high serum HBsAg titers were originally shown to provide a supply of viral antigen for the production of the first commercially available form of the vaccine. This achievement was crucial to the overall effort because hepatitis B virus has not yet been routinely cultured in vitro.
Ultracentrifugation was found to be a very effective means for large-scale isolation of HBsAg from asymptomatic hepatitis B carriers. Additional chemical treatment of the isolated surface proteins with the enzyme pepsin, concentrated urea, and formalin was designed to inactivate any residual HBV particles or particles of any other possible virus, and to remove any residual traces of plasma protein as well. These measures produced a vaccine suitable for administration to human beings.
With refinement of the original vaccine (addition of alum as an adjuvant to increase vaccine immunogenicity), it became apparent that an effective prophylactic weapon had been developed. One of the clinical trials with this vaccine assessed its efficacy in a placebo-controlled, randomized, double blind study in 1983 with homosexual men known to be at high-risk for hepatitis B. The vaccine was found to induce high titers of anti-HBs in injected persons (77 percent after primary dose, 96 percent after booster). Of prime importance was the observation that during an 18-month follow-up interval, 18 to 27 percent of the placebo recipients developed clinical or subclinical hepatitis B while only 1.4 to 3.4 percent of the HBsAg-vaccinated subjects did so.
Heptavax-B, the vaccine (Merck and Company), was released for commercial use in 1982. This preparation is a sterile suspension for intramuscular injection. Each 1.0 ml dose of vaccine contains 20 μg of hepatitis B surface antigen formulated in an alum adjuvant, and thimerosal (a mercury derivative) 1:20,000 as a preservative. It was used for immunization against all known subtypes of hepatitis B virus, but did not prevent infection caused by hepatitis A, hepatitis C,
or hepatitis E viruses. Subsequent infection with HDV was prevented, however, as hepatitis D cannot develop in individuals who are protected from hepatitis B infection.
The preparation is given in a regimen of three 1.0 ml intramuscular doses. The second and third doses are given at one and six months, respectively, following the first injection. No serious side effects have been attributed directly to parenteral injection of the vaccine. Mild, short-term effects include soreness at the injection site, fever, flu-like symptoms, and general malaise. With the development, approval, and marketing of second-generation hepatitis B vaccines, which do not use plasma from HBV carriers, the original Heptavax-B is currently available only in limited amounts and is reserved for patients with specific medical conditions.
Recombinant (Single-Antigen) DNA Vaccines
The first clinical vaccine prepared using recombinant (produced from a cloned gene) DNA technology was licensed in 1986 and made available for general use in 1987. Recombivax HB (Merck and Company) was developed initially as a newer vaccine to provide an alternative to the plasma-derived vaccine.
This preparation is produced in cultures of Saccharomyces cerevisiae (common baker's yeast), into which a plasmid containing the gene for HBsAg has been inserted. HBsAg is subsequently harvested after lysis of cultured yeast cells. Administered vaccine is designed to contain 10 micrograms (μg) of HBsAg protein per milliliter, absorbed with 0.5 milligrams per ml of aluminum hydroxide (alum), with thimerosal as a preservative.
The immunogenicity of Recombivax HB is comparable to that observed for the plasma-derived preparation. In 1989 Smith, Kline, Beecham received a license in the U.S. for their Engerix-B vaccine. The major difference between the products is the number of steps used in recovery and purification of the antigen from the yeast cultures, which results in different dosage amounts. Both vaccine preparations provide adequate immunity. Table 1 includes a chart of the recommended dosage and timeline for receiving the hepatitis B vaccines.
Combination Vaccines
Combination vaccines have been developed that combine an HBV vaccine with other vaccines. The Comvax, Pediarix, and Twinrix combination vaccines have been combined with other vaccines to reduce the number of injections for infants and children. See Table 1 for recommended dosages and timelines.
Testing for Immunity
After receiving a series of hepatitis B vaccinations, the individual should receive a blood test (anti-body titer) to verify their immunity. Most will sero-convert after receiving the standard recommended protocol. However, there are cases when a person will not receive immunity and will need an additional injection, or even a repetition of the full series.
For an adult, the titer should be drawn 1 - 2 months after the series was completed. When the results are returned, the results should come back showing that the worker is positively immune to hepatitis B. Unfortunately, laboratory results can be worded differently and can be misinterpreted. Table 2 can be used to interpret received results.
RECOMMENDATIONS FOR INFECTION CONTROL PROCEDURES
This course was not designed to provide a comprehensive section on infection control precautions. However, it is appropriate to include a summary description of current infection control recommendations.
Effective infection control must occur as a routine component of professional activity. The use of standard precautions to manage all patients minimizes occupational exposure to microbial pathogens by addressing the reality that most potentially infectious individuals are asymptomatic and therefore undiagnosed. This has already been discussed in terms of various types of viral hepatitis. The medical history should not be used to definitively identify the "infectious disease risk" of a patient. For that reason, every patient must be considered infectious and the same infection control procedures applied for all patients. Unfortunately, this concept of standard precautions is a difficult one for some dental professionals to put into practice. However, when standard precautions are used, additional procedures are not necessary when treating a patient who is known to have an infectious disease.
The importance of these precautions in applying professional organization recommendations, Centers for Disease Control and Prevention guidelines, and the OSHA standard must be considered. Develop an organized, comprehensive program with input from all dental professionals in the clinical setting. Determine the infection control strengths of your practice and build on them by integrating new knowledge into the practice routine.
SUMMARY
A range of hepatitis infections can be obtained through many means including routine tasks in a dental office. It is important for dental professionals to be aware of these infections and their symptoms as well as the modes of transmission. The change from the initial 1978 ADA recommendations to the present has been great, and other modifications probably will be made for the next few years. It is therefore essential for dental professionals to remain current on this topic, as developments in infection control continue to provide better products and advances in asepsis technology.
HEPATITIS C: General Information
What is hepatitis?
"Hepatitis" means inflammation of the liver. The liver is a vital organ that processes nutrients, filters the blood, and fights infections. When the liver is inflamed or damaged, its function can be affected.
Hepatitis is most often caused by a virus. In the United States, the most common types of viral hepatitis are hepatitis A, hepatitis B, and hepatitis C. Heavy alcohol use, toxins, some medications, and certain medical conditions can also cause hepatitis.
What is hepatitis C?
Hepatitis C is a contagious liver disease that results from infection with the hepatitis C virus. When first infected, a person can develop an "acute" infection, which can range in severity from a very mild illness with few or no symptoms to a serious condition requiring hospitalization.
Acute hepatitis C is a short-term illness that occurs within the first 6 months after someone is exposed to the hepatitis C virus. For reasons that are not known, 15%-25% of people "clear" the virus without treatment. Approximately 75%-85% of people who become infected with the hepatitis C virus develop "chronic," or lifelong, infection.
Chronic hepatitis C is a long-term illness that occurs when the hepatitis C virus remains in a person's body. Over time, it can lead to serious liver problems, including liver damage, cirrhosis, liver failure, or liver cancer (see chart).
How is hepatitis C spread?
Hepatitis C is usually spread when blood from a person infected with the hepatitis C virus enters the body of someone who is not infected. Today, most people become infected with hepatitis C by sharing needles or other equipment to inject drugs. Before widespread screening of the blood supply began in 1992, hepatitis C was also commonly spread through blood transfusions and organ transplants. Although uncommon, outbreaks of hepatitis C have occurred from blood contamination in medical settings.
Can hepatitis C be spread through sex?
Yes, although scientists do not know how frequently this occurs. Having a sexually transmitted disease or HIV, sex with multiple partners, or rough sex appears to increase a person's risk for hepatitis C. There also appears to be an increased risk for sexual transmission of hepatitis C among gay men who are HIV-positive.
Can a person get hepatitis C from a tattoo or piercing?
There is little evidence that hepatitis C is spread by getting tattoos in licensed, commercial facilities. Whenever tattoos or body piercings are given in informal settings or with non-sterile instruments, transmission of hepatitis C and other infectious diseases is possible.
Can hepatitis C be prevented?
Yes. To reduce the risk of becoming infected with the hepatitis C virus:
• Do not share needles or other equipment to inject cosmetic substances, drugs, or steroids
• Do not use personal items that may have come into contact with an infected person's blood, such as razors, nail clippers, toothbrushes, or glucose monitors
• Do not get tattoos or body piercings from an unlicensed facility or in an informal setting
Is there a vaccine for hepatitis C?
Although there is currently no vaccine to prevent hepatitis C, research is being conducted to develop one.
How common is hepatitis C?
An estimated 3.2 million people in the United States have chronic hepatitis C. Most are unaware of their infection. Each year, about 17,000 Americans become infected with hepatitis C.
How serious is hepatitis C?
Chronic hepatitis C is a serious disease that can result in long-term health problems, including liver damage, liver failure, and liver cancer. Approximately 12,000 people die every year from hepatitis C-related liver disease.
What are the symptoms of hepatitis C?
Many people with hepatitis C do not have symptoms and do not know they are infected. Even though a person has no symptoms, the virus can still be detected in the blood.
If symptoms occur with acute infection, they can appear anytime from 2 weeks to 6 months after exposure. Symptoms of chronic hepatitis C can take up to 30 years to develop. Damage to the liver can silently occur during this time. When symptoms do appear, they often are a sign of advanced liver disease. Symptoms for both acute and chronic hepatitis C can include fever, fatigue, loss of appetite, nausea, vomiting, abdominal pain, dark urine, grey-colored stools, joint pain, and jaundice.
How is hepatitis C diagnosed?
Doctors can diagnose hepatitis C using specific blood tests that are not part of blood work typically done during regular physical exams. Typically, a person first gets a screening test that looks for "antibodies" to the hepatitis C virus. Antibodies are chemicals released into the bloodstream when a person becomes infected. The antibodies remain in the bloodstream, even if the person clears the virus. If the screening test is positive for hepatitis C antibodies, different blood tests are needed to determine whether the infection has been cleared or has become a chronic infection.
Who should get tested for hepatitis C?
Testing for hepatitis C is recommended for certain groups, including people who:
• Currently inject drugs
• Injected drugs in the past, even if it was just once or occurred many
• years ago
• Have HIV infection
• Have abnormal liver tests or liver disease
• Received donated blood or organs before 1992
• Have been exposed to blood on the job through a needlestick or
• injury with a sharp object
• Are on hemodialysis
How is hepatitis C treated?
Since acute hepatitis C rarely causes symptoms, it often goes undiagnosed and therefore untreated. When it is diagnosed, doctors recommend rest, adequate nutrition, fluids, and antiviral medications. People with chronic hepatitis C should be monitored regularly for signs of liver disease. Even though a person may not have symptoms or feel sick, damage to the liver can still occur. Antiviral medication can be used to treat some people with chronic hepatitis C, although not everyone needs or can benefit from treatment. For many, treatment can be successful and results in the virus no longer being detected.
What can people with hepatitis C do to take care of their liver?
People with chronic hepatitis C should see a doctor regularly. They also should ask their health professional before taking any prescriptions or over-the-counter medications-including herbal supplements or vitamins-as they can potentially damage the liver. People with chronic hepatitis C should also avoid alcohol since it can accelerate liver damage.
For more information
Talk to your health professional, call your health department, or visit www.cdc.gov/hepatitis.
DEPARTMENT OF HEALTH & HUMAN SERVICES
Centers for Disease Control and Prevention
Division of Viral Hepatitis
Publication No. 21-1075
June 2010
GLOSSARY
Acute - short term and/or severe.
Adjuvant - one drug added to anther to enhance the effectiveness.
Anicteric - not associated with jaundice.
Antibody - specific protein produced by the immune system as a reaction to the presence of an antigen.
Antigen - substance which is capable, under appropriate conditions, of inducing a specific immune response and of reacting with the products of that response.
Asymptomatic - absence of symptoms.
Bilirubin - reddish-yellow organic compound derived from hemoglobulin during normal and pathological destruction of erythrocytes.
Carrier - individual harboring a disease agent, who may transmit the infection, without demonstrating apparent symptoms.
Chronic - long duration, may or may not be severe.
Cirrhosis - chronic liver disease characterized by progressive destruction and regeneration of liver cells and increased connective tissue formation.
Etiology - cause of a disease.
Fibrosis - formation of tissue composed of or containing fibers.
Fulminant - occurring suddenly, rapidly, and with great intensity, high mortality rate.
Gamma globulin - generally any serum protein exhibiting antibody activity.
Hemodialysis - removal of certain elements of the blood by virtue of the difference in the rates of their diffusion through a semipermeable membrane.
Hepatitis - inflammation of the liver. Icteric - relating to or marked by jaundice.
Inflammation - fundamental pathologic process which occurs following any injury to tissue, such as that following the establishment and multiplication of microorganisms.
In vitro - studies performed under artificial conditions. In vivo - in the living body or organism.
Jaundice - yellowish staining of the skin, mucous membranes, and sclera with bilirubin and other bile pigments.
Malaise - vague feeling of general body discomfort and uneasiness.
Necrosis - sum of the morphological changes indicative of cell death and caused by the progressive degradative action of enzymes.
Parenteral - not through the alimentary canal but rather by injection through some other route.
Percutaneous - performed through the skin.
Prodromal - indicating the initial stage of a disease.
Recombinant vaccine - suspension of attenuated or killed microorganisms administered for the prevention of disease.
Sequelae - condition following as a consequence of another disease.
Subclinical infection - state in which the individual either does not experience all of the characteristic symptoms of a particular disease, or the manifestations are less severe.
Viremia - presence of viruses in the blood.
Virion - complete virus particle.
REFERENCES
1. Molinari, J.A. and Merchant, V.A. Viral Hepatitis - An Occupational Disease. Dent. Assistant. 52:25, 1983.
2. Notice to Readers. Licensure of Inactivated Hepatitis A Vaccine and Recommendations for Use Among International Travelers. MMWR 44(29);559-560. July 28, 1995
3. Prevention of Hepatitis A Through Active or Passive Immunization: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 48(RR12) 37 October 01, 1999
4. Updated US Public Health Service Guidelines for the Management of Occupational Exposure to HBV, HCV, and HIV and Recommendations for Postexposure Prophylaxis MMWR 50 (RR11); 1-42 June 29, 2001
5. Krugman, S. Perspectives on Viral Hepatitis #4. Prophylaxis of Hepatitis B. Hepatitis Information Center. Abbott Laboratories, Diagnostic Division, North Chicago, IL, 1983.
6. Gitnick, G. Non-A, Non-B Hepatitis: Etiology and Clinical Course. Ann. Rev. Med. 35:256, 1984.
7. Hoofnagle, J.H. Perspectives on Viral Hepatitis #2. Types A and B Viral Hepatitis. Hepatitis Information Center. Abbott Laboratories, Diagnostics Division, North Chicago, IL 1983.
8. Martin, C.M. Hepatitis B Vaccine: What to Expect. Oral Surg. 56:455, 1983.
9. Szmuness, W., et al. Hepatitis B Vaccine. Demonstration of efficacy in a controlled clinical trial in a high-risk population in the United States. New Eng. J. Med. 303:833, 1980.
10. Herron, W.; Petersohn, E.; and Taylor, J.W. Non-A, Non-B Hepatitis infection transmitted via a needle-Washington. MMWR 28:157, 1979.
11. Tabor, E., Seeff, L.B., and Gerety, R.J. Chronic Non-A Non-B Hepatitis carrier state. Transmissible agent documented in one patient over a six-year period. New Eng. J. Med. 303:140, 1980.
12. Perrillo, R.P., and Aach, R.D. The clinical course and chronic sequelae of hepatitis B virus infection. Seminars in Liver Disease 1:15-25, 1981.
13. Goebel, W.M. Reliability of the medical history in identifying patient likely to place dentists at an increased hepatitis B virus infection. JADA 98:907, 1979.
14. Tullman, M.J.; Boozer, C.H.; and Vallarejos, V.M., et al. The threat of hepatitis B from dental school patients. Oral Surg. 49:214, 1980.
15. Viral Hepatitis type B, tuberculosis, and dental care of Indochinese refugees. MMWR 29:1, 1980.
16. Rimland, D.; Parkins, W.E.; Miller, G.B., et al. Hepatitis B outbreak traced to an oral surgeon. New Eng. J. Med. 296:953, 1977.
17. Immunization practices advisory committee. Inactivated Hepatitis B virus vaccine. MMWR 31:317, 1982.
18. Update on Adult Immunization. Recommendations of the Immunization Practices Advisory Committee (ACIP) MMWR, 1991.
19. Epidemiologic Notes and Reports. Enterically Transmitted Non-A, Non-B Hepatitis - Mexico. MMWR, 1987.
20. Cooper, B.W., Krusell, A, Tilton, R., Goodwin, R., Levitz, R., et al. Seroprevalence of Antibodies to Hepatitis C Virus in High- Risk Hospital Personnel. If. Control. & Hosp. Immune. 13:82, 1992.
21. Cottone, J.A., Molinari, J.A., State of the Art Infection Control in Dentistry. JADA 123:33, 1991.
22. Polish, L.B., Gallagher, M., Fields, H.A., Hadler, S.C.: Delta Hepatitis: Molecular Biology and Clinical and Epidemiological Features. Cl. Micro. Rev. 6:211, 1993.
23. Cottone, J.A. Delta hepatitis: Another Concern for Dentistry. JADA 112:47, 1986.
24. Epidemiologic Notes and Reports - Hepatitis E Among U.S. Travelers, 1989-1992. MMWR, Jan. 1993.
25. Schuster, G.S. Oral Microbiology & Infectious Disease. Third Ed. B.D. Decker, 1990.
26. Cottone, J.A., Terezhalmy, G.T., Molinari, J.A. Practical Infection Control in Dentistry. Lea & Febiger, 1991.
27. http://www.cdc.gov/ncidod/diseases/hepatitis/a/index.htm Accessed 4/24/20
28. http://www.cdc.gov/ncidod/diseases/hepatitis/b/index.htm Accessed 4/24/20
29. http://www.cdc.gov/ncidod/diseases/hepatitis/c/index.htm. Accessed 4/24/20
30. http://www.cdc.gov/ncidod/diseases/hepatitis/d/fact.htm Accessed 4/24/20
31. Little, J.W. Recent advances in the treatment of viral hepatitis. General Dentistry. Nov/Dec, 2000.
32. http://www.cdc.gov/hepatitis/HBV/HBVfaq.htm#vaccFAQ Accessed 4/24/20
33. http://www.cdc.gov/hepatitis/Statistics/index.htm. Accessed 4/24/20
34. http://www.cdc.gov/hepatitis/b/bFAQ.htm. Accessed 4/24/20
35. http://www.cdc.gov/Hepatitis/HCV/HCVfaq.htm#a6. Accessed 4/24/20
36. http://www.healthcare.com/search-results/?cx=partner-pub- 1999919262198914%3A1389059887&cof=FORID%3A10&ie= UTF-8&q=hepatitis+c&sa=Search&siteurl=www.healthcare. com%2F&ref=&ss=3111j1499623j11. Accessed 7/21/2014.
37. http://www.fda.gov/forconsumers/byaudience/ forpatientadvocates/ucm377920.htm. Accessed 7/21/2014.
38. http://www.ada.org/en/publications/ada-news/2013-archive/ september/one-confirmed-hepatitis-c-infection-in-ongoing- investigation-of-tulsa-dental-office. Accessed 7/17/2014.
ABOUT THE AUTHORS
John A. Molinari, Ph.D.
Dr. Molinari received a B.A. in Biology from St. Vincent College and a Ph.D. in Microbiology from the University of Pittsburgh, School of Dental Medicine. He is currently Director of Infection Control for THE DENTAL ADVISOR. Previously, he served for 32 years at the University of Detroit Mercy School of Dentistry as Professor and Chairman of the Department of Biomedical Sciences and Director of Infection Control. He has published over 350 scientific articles, text chapters, and abstracts in the areas of microbiology and immunology, and lectures nationally and internationally on topics dealing with infectious diseases and infection control. Dr. Molinari is also co-author of the text Cottone's Practical Infection Control in Dentistry, with the 3rd edition published in 2009. He was a founding member of the Organization for Safety, Asepsis and Prevention (OSAP) and received that organization's highest honor, the Dr. James Crawford Award, for his lifetime achievement in the fields of infection prevention and safety. His activities also include serving as a consultant for the CDC, ADA Council on Scientific Affairs, Council on Dental Practice, and hospitals in the Detroit area in the areas of infectious disease and infection control. Previously, he was the Project Coordinator for the governmental Health Resources and Services Administration Task Force on AIDS and Dental Education, as well as Chairman of the American Association of Dental School's Curriculum Advisory Committee on Bloodborne Infectious Diseases. Dr. Molinari also was appointed and served as Chairman of the State of Michigan Governor's Risk Reduction and AIDS Policy Commission. He was the Infection Control section editor for The Compendium of Continuing Education in Dentistry and a member of the Editorial Board for The Journal of the American Dental Association. He currently writes a monthly column for Dental Economics. In recognition of his efforts, Dr. Molinari was inducted as an honorary member of the Michigan Dental Association, the International College of Dentists, the American College of Dentists, and is a 2009 recipient of the ADA Golden Apple Award.
Eve Cuny, RDA, MS
Ms. Cuny received her BA in management and MS in Health Services Administration from Saint Mary's College of California. She is the Director of Environmental Health and Safety and Assistant Professor, Department of Dental Practice at the University of the Pacific School of Dentistry in San Francisco, CA. Ms. Cuny has published numerous textbook chapters and articles in the scientific literature. She lectures extensively in the United States and Latin America on infection control and regulatory compliance. Ms. Cuny has acted as advisor or reviewer for the California Dental Association, the California Dental Board, the Centers for Disease Control and Prevention, and the American Dental Association. She is past Chairperson and a previous board member for the Organization for Safety and Asepsis Procedures (OSAP).