You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
INITIAL DATA GATHERING
Utilizing an organized, consistent protocol for gathering periodontal clinical data is the key to efficiency and effectiveness in planning treatment for the patient.
The diagnostic data that is gathered at the initial appointment should include:
1. A current medical history questionnaire/form that is signed and dated by the patient and dentist.
2. Information about previous dental treatment including periodontal visits and maintenance instructions. (This may be acquired by an interview of the patient or by using a pre-printed list of questions.)
3. Radiographs, both past and present.
4. Clinical charting, both past and present.
Frequently, patients are referred to the dental office after relocation or when they decide to change dentists for various reasons. Most dental offices are very cooperative about sending records when requested to by a former patient or the new dentist. It is best to contact the dental office after the new patient calls for their first appointment, thereby allowing time in the initial appointment to take new radiographs if the most recent films are not current.
Collecting and organizing clinical data can be a simple process once the significant steps are identified. These steps must be followed in the same sequence with every patient, every time a patient is seen. It is imperative to use an organized, systematic approach for each patient. Do not skip steps and always be sure to follow all HIPAA regulations.
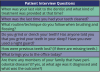
Patient Interview
The patient interview is the first step. It is the most important step in gaining the patient's confidence and trust and is also the best source of data gathering available. Asking open-ended questions and listening carefully to the patient's answers provides information needed to assess a possible periodontal problem. Patients with moderate stage periodontal disease often complain of "bad breath." This is frequently noticed by someone other than the patient himself or herself and may be one of the primary reasons that they requested the appointment. Some patients notice bleeding when brushing and flossing and this may be another reason that they seek dental care.
The patient interview can provide valuable data. Examples of appropriate questions are included in Table 1.
Medical/Dental History
The medical history (Figure 1) is used to evaluate the patient's potential to have systemic diseases that would contribute to the periodontal condition.
A thorough patient interview to review the answers given on the medical history form is important because patients frequently do not understand the relationship between their medical problems and medications and their overall dental health. Often the reverse is also true. They may not understand that their oral health can affect their overall physical health. Periodontal disease can be a symptom of several systemic diseases. Consultation with the patient's physician may be the first step of treatment.
Diseases and conditions such as hypertension, diabetes, heart disease, respiratory conditions, pregnancy, and AIDS, for example, can have a direct effect on the periodontium. Use of tobacco products is extremely detrimental to the periodontium. Many dentists require the patient to complete a tobacco cessation program before periodontal treatment is begun.
The complete history should include:
• any background information about oral complaints from the patient
• an updated medical history including any new medical conditions and medications
• family and social history
Documents relating to the medical and dental history should be reviewed at each appointment. All notations should be written into the chart and signed and dated by the clinician and the patient.
The importance of medical and dental histories cannot be overemphasized. Not only do they provide information about the patient, but they also promote interaction that leads to trust and better patient compliance.
RADIOGRAPHIC EVALUATION FORPERIODONTAL DISEASE
Intraoral radiographs aid in the detection of periodontal disease. A complete set of current radiographs is essential to the dentist for making decisions concerning treatment planning and diagnosis. Although radiographic needs should be evaluated on a patient-by-patient basis, most adults require a complete full mouth series, including four posterior vertically oriented bitewings. Panoramic surveys and horizontal bitewings do not provide an accurate diagnostic tool for evaluating the periodontal condition.
Radiographs provide clinical evidence and data that will determine the treatment for the patient and affect the outcomes of the disease. The data that can be observed on radiographs is denoted on Table 2.
The radiographs should also be reviewed to evaluate the type and degree of bone loss. This judgment is based on the amount of available bone in relationship to the root. The significance of the bone loss would vary depending on the length of the root.
Full-mouth radiographs should be taken every three to five years based on the patient's specific needs.
Vertical bitewings should be taken yearly. Placing the bitewings in an orderly fashion in the mount allows comparison and contrast from one year's radiographs to the next. Digital imaging systems are especially useful with their capacity to store a chronological series of radiographs and display them for comparison.
Even though dental radiographs are important documents of the patient's history of dental disease, the films only tell you what has occurred, not when it occurred. Other limiting characteristics of radiographic use in diagnosis and prognosis of periodontal disease include:
• lack of buccal and lingual views of the alveolar bone
• the variation in appearance of periodontal ligament space
• two-dimensional distortion of overlapping anatomical structures
• inability to locate soft tissue margins
Radiographs also do not reveal minimal losses of bone. In fact, for bone loss to be diagnosed from a radiograph, 40% bone loss must have already occurred.
The use of high kVp during radiographic exposure produces a longer scale of contrast and is often preferred in detecting periodontal disease.
PERIODONTAL EVALUATION FOR DISEASE
When performing any part of the periodontal examination, it is very important to look for the early signs of disease activity. Bleeding upon probing is one of the earliest manifestations of possible periodontal disease.
Disease activity is a frequently misused term. It is defined as a disease process resulting in attachment/bone loss. Active destruction of the periodontium is occurring. Bleeding upon probing may be present with or without disease activity and the absence of bleeding upon probing does not necessarily indicate an inflammation-free site or a healthy oral environment. Pocket depth measurements are essential for providing the baseline assessments from which treatment plan, treatment progress, and continue care maintenance can be monitored.
PERIODONTAL PROBES
Various types of periodontal probes can be used to measure pocket depths. Most clinicians use their own personal preferences in determining which probe to use.
Types of Probes
Most traditional probes are marked with 1-millimeter increments with the 4 and 6 mm marking absent. Many dental hygiene clinical boards require proficiencies with a probe reading 1, 2, 3, 5, 7, 8, 9, and 10 mm. Some probes have a black band indicating the 3, 5, 9, and 10-mm markings. Other probes are marked at 3mm. Some clinicians prefer probes that are color coded because they are easier to read.
The Naber's probe or the Furcation probe is a blunt ended instrument that is used buccally and lingually on the periodontal structure to locate possible furcation involvement.
Periodontal Probing Guidelines
Since periodontal probing is such an important aspect of the periodontal examination, the technique must be systematic and consistent (Table 3). The operator, when probing, will:
• Use a lateral "walking" approach
• Use only one brand of probe to achieve standardization
• Dictate findings to the dental assistant or a software activated program who will chart data on a form that allows comparison of readings over time
• Record six regions around each tooth
Even though periodontal probing is one of the best diagnostic tools we have to assess periodontal disease, there are also certain pitfalls to avoid:
• Subgingival calculus can interfere with accurate readings
• In an area with elevated inflammation, the attachment is easily perforated
• The pocket may be too tight to probe
• The patient may present with hypersensitivity making accurate probing difficult
Visibility is another extremely important factor in accurate probing. It is important that the probe be clearly visible to obtain accurate results. The skillful use by the dental assistant of the air/water syringe and the evacuation system will help keep the probing areas visible.
Bleeding at the gingival margin or sulcus is often the first indicator of gingivitis or periodontitis. Bleeding, pocket depths, and radiographs are used together to determine the periodontal condition. These measurements are significant for two different types of periodontal disease and their future treatment.
GINGIVAL RECESSION
Gingival recession is important to the periodontal examination because it accurately indicates the total amount of attachment loss. Attachment loss can vary from tooth to tooth. Any tooth can have attachment loss without having a pocket.
The amount of attached gingiva can be calculated by subtracting the probing depth from the width of the keratinized gingiva. Tissue color for keratinized tissue is lighter pink with a stippled appearance.
MOBILITY CLASSIFICATIONS
Mobility is an indicator of bone loss around the tooth. In order to accurately evaluate mobility, two non-working ends of the dental instruments (i.e., the mirror handle and the probe handle) are pressed on the buccal and lingual surfaces of the tooth. The amount of movement is measured and classified as:
Class O - Complete tooth stability.
Class I - Slight mobility, up to 1 mm of displacement in any direction.
Class II - Moderate mobility, greater than 1 mm but less than 2 mm but is not depressible into the socket.
Class III - Severe mobility, greater than 2 mm of displacement and is depressible into the socket.
FURCATION CLASSIFICATIONS
Furcation involvement indicates a serious periodontal condition that if detected early is treatable with guided tissue regeneration.
Frequently, the areas that are most vulnerable to furcation involvement (the posterior areas of the mouth) are difficult to access. As a result, abscesses, progressive attachment loss and deep periodontal pockets may develop and be undetected.
The four classes of furcation involvement that are identified with the Naber's probe are:
Class I - the furcation can be probed to a depth of 3 mm. Using the probe, the anatomic fluting between the roots can be felt, but cannot engage the roof of the furcation.
Class II - the furcation can be probed to a depth greater than 3 mm, but not through and through.
Class III - The furcation can be completely probed through and through subgingivally.
Class III+ - Naber's probe can go halfway across the tooth.
Class IV - The probe goes completely through the furcation and is supragingival.
Furcation probing is significant because most teeth lost to periodontal disease are multi-rooted teeth. It is absolutely essential to evaluate the furcation of these teeth. The classification of the involvement affects the choice of instruments that are used for debridement. The goal is to get the probe under the furcation, classify it and chart it.
SUMMARY
The assessment and evaluation of the periodontal status of the patient involves the use of a thorough medical and dental history, radiographs, periodontal charting to include pocket depth, and mobility and furcation involvement. From these clinical findings, the type of periodontal disease can then be diagnosed by the dentsit and the appropriate treatment can be initiated. The earlier the detection and appropriate therapy is initiated, the less chance there will be for tooth loss.
About the Authors
Members of the 2001-2002 ADAA Council on Education originally developed this course. All members of the Council on Education are ADAA Active or Life Members with an interest in dental assisting education. Each one volunteers their time to the life long learning of dental assistants.
The 2005- 2006 ADAA Council on Education updated this course.
The 2010-2011 ADAA Council on Education updated this course.
The 2019-2020 ADAA Council on Education and Professional Development updated this course.
References
Classification, Epidemiology, and Diagnosis of Periodontal Diseases Study Club Kit, http://www.perio.org/commerce05/pdf/ced.pdf, accessed on 4.24.10
HuFriedy Manufacturing Company, Inc. Product Catalog & Reference Guide. Chicago: 4th Edition: 6-10.
Jaroski-Graf J. Dental Charting: A Standard Approach. Albany; Delmar, 2000: 38, 291-293, 216 - 223.
Bird D; and Dietz E. (2009) Torres & Erlich's Modern Dental Assisting. 9th Ed., St. Louis, Sauders Elsevier.
Weinberg MA, et.al. (2009) Comprehensive Periodontics for the Dental Hygienist; 3rd Ed., pg. 226
Bird D, Robinson D. (2018) Modern dental assisting. St. Louis, MO: Elsevier.